Have you ever wondered why your eye doctor consistently asks whether you have a cat at home during routine examinations? Perhaps you have noticed an unusual shadow drifting across your field of vision that was not there before? There exists a parasitic infection affecting over two billion people worldwide, with many individuals completely unaware they harbor this organism. This condition is known as ocular toxoplasmosis, and understanding its mechanisms, symptoms, and treatment options could be crucial for protecting your vision.
Throughout this article, we will explore what ocular toxoplasmosis truly is, examine how it causes damage to your eyes, identify the symptoms requiring immediate attention, and most importantly, discuss the treatment options available to safeguard your precious vision.
What Is Ocular Toxoplasmosis and What Causes It?
Before exploring the specific details of how this condition affects vision, it helps to understand the fascinating yet concerning nature of the organism responsible. Ocular toxoplasmosis results from infection by a microscopic parasite called Toxoplasma gondii, a single-celled organism that ranks among the most successful parasites known to science. Recent research indicates that this parasite has infected approximately one-third of the global human population, making it remarkably widespread.
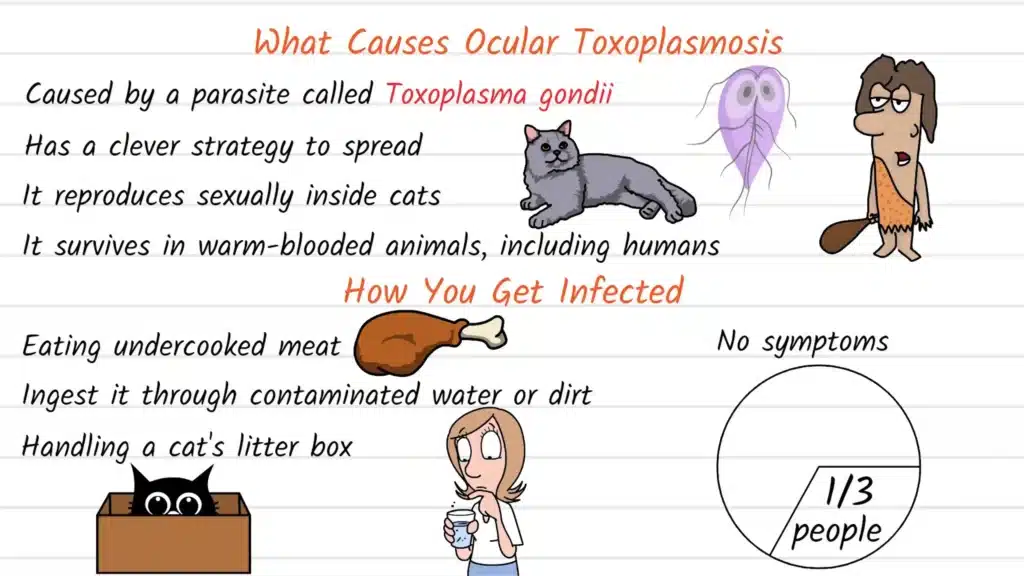
The remarkable success of Toxoplasma gondii stems from its sophisticated survival and transmission strategy. This parasite can only complete its sexual reproductive cycle within cats, which serve as its definitive host. However, the organism demonstrates remarkable adaptability by surviving in virtually any warm-blooded animal, including humans, birds, livestock, and many other mammals. This dual-host strategy ensures the parasite’s continued propagation across diverse environments and species.
According to data from community-based studies conducted in various regions, the prevalence of ocular manifestations varies significantly by geographic location. In the United States, approximately 2% of those infected with Toxoplasma gondii develop ocular disease, while in certain regions of Brazil, this figure can reach as high as 18%, and in some African locations, up to 43% of infected individuals experience eye involvement.
Understanding How Infection Occurs
The transmission pathways for Toxoplasma gondii infection are more common than most people realize, which partly explains the parasite’s widespread prevalence. One primary route involves consuming undercooked or raw meat containing tissue cysts of the parasite. Pork, lamb, and venison represent particular risk sources, although proper cooking at adequate temperatures eliminates this danger entirely.
Another significant transmission route occurs through accidental ingestion of oocysts, which are hardy, environmentally resistant forms of the parasite shed in cat feces. This can happen when individuals handle cat litter boxes without thorough hand washing afterward, work in gardens or soil contaminated with cat feces, or consume unwashed fruits and vegetables exposed to contaminated soil or water sources.
Many individuals contract toxoplasmosis through these routes without developing any noticeable symptoms whatsoever. In fact, epidemiological studies suggest that approximately one in three people globally carries this infection, though the vast majority never experience problems specifically related to their eyes. The infection typically remains dormant within tissue cysts throughout various body locations, including muscle tissue, the brain, and occasionally, the eyes.
The Mechanism of Eye Damage in Ocular Toxoplasmosis
When Toxoplasma gondii parasites somehow migrate to ocular tissues, the condition termed ocular toxoplasmosis develops. This manifestation is particularly concerning because the infection characteristically attacks the retina, the delicate, light-sensitive tissue lining the back interior surface of your eye. The retina serves the critical function of capturing incoming light and converting it into electrical signals that travel through the optic nerve to your brain, where these signals are interpreted as visual images.
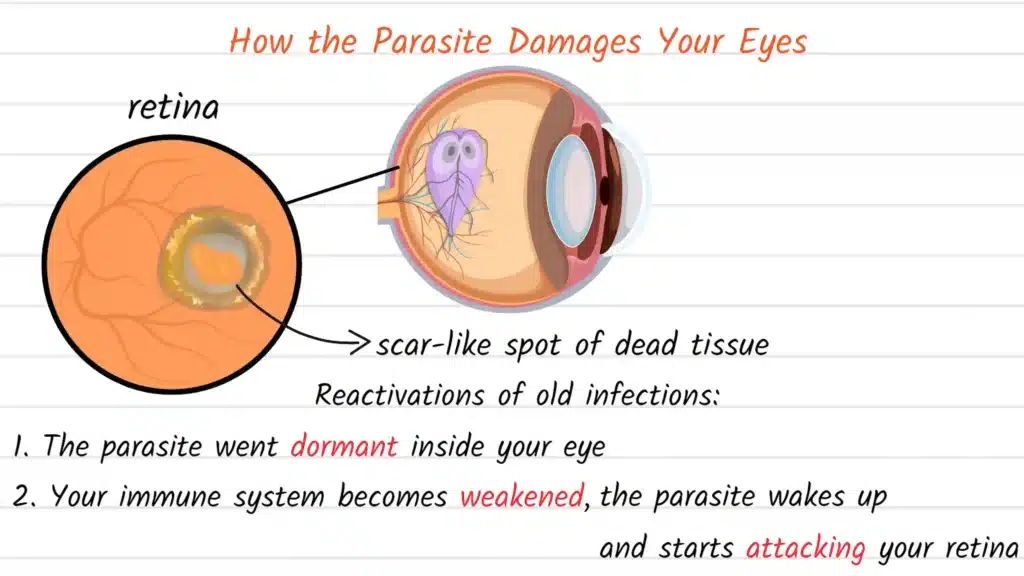
When parasites invade retinal tissue, they trigger an inflammatory response as your immune system attempts to eliminate the infection. This inflammation creates what ophthalmologists call a lesion, which essentially represents an area of damaged, necrotic (dead) tissue that subsequently scars over. The location, size, and number of these lesions directly determine the impact on visual function.
What makes ocular toxoplasmosis particularly challenging is that most cases represent reactivations of old, previously acquired infections rather than new, acute infections. The parasite can remain dormant within retinal tissue for years or even decades without causing problems. Then, when circumstances change, particularly if your immune system becomes weakened or compromised for any reason, the dormant parasites reactivate and begin multiplying again, creating new inflammation and additional retinal damage.
This pattern of dormancy followed by reactivation explains why individuals with compromised immune systems face substantially higher risk. People living with HIV/AIDS, those receiving immunosuppressive medications following organ transplants, patients undergoing chemotherapy, and individuals with certain autoimmune conditions requiring immunosuppressive treatment all experience elevated risk of active ocular toxoplasmosis.
Recognizing the Symptoms of Ocular Toxoplasmosis
Early recognition of ocular toxoplasmosis symptoms proves crucial for preventing permanent vision damage. The condition presents with various symptoms depending primarily on the location and size of the retinal lesion. Many individuals with ocular toxoplasmosis report experiencing floaters, which appear as tiny dark spots, threads, or cobweb-like shapes that seem to drift across the field of vision. These floaters result from inflammatory cells and debris floating within the vitreous humor, the gel-like substance filling the interior of your eye.
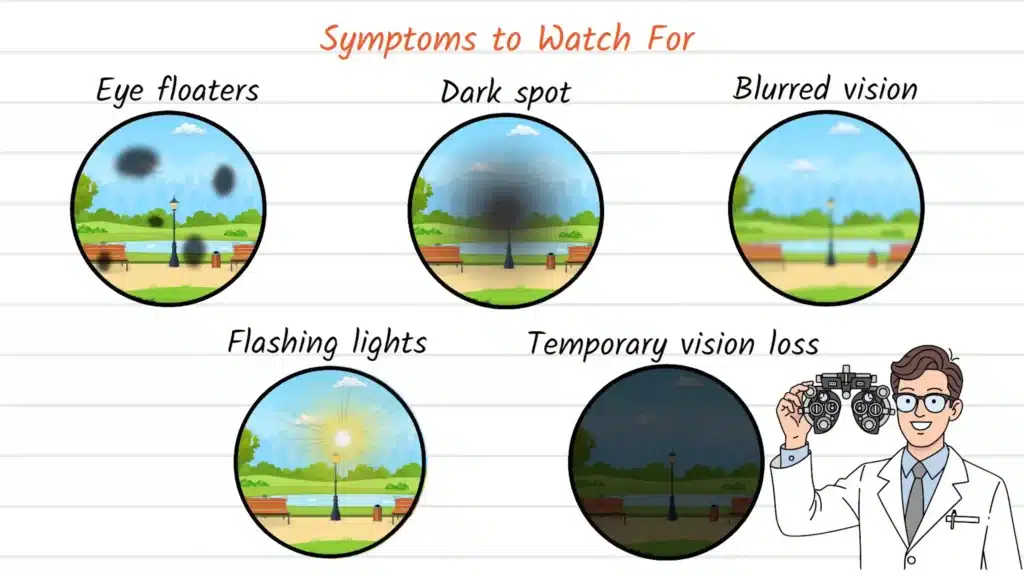
Beyond floaters, you might notice a shadow or persistent dark spot affecting a specific area of your vision, particularly if the inflammatory lesion involves your central visual field or macular region. The macula represents a small but critically important area of the retina responsible for sharp, detailed central vision needed for activities like reading, driving, and recognizing faces. When lesions affect this region, the visual consequences become significantly more severe.
Additional symptoms can include distinctly blurred or distorted vision, where straight lines may appear wavy or objects seem misshapen. Some patients experience photophobia, an uncomfortable sensitivity to light. In more severe or rapidly progressing cases, individuals might perceive flashing lights, particularly in peripheral vision, or experience episodes of sudden, temporary vision loss.
The crucial point to understand is that if you experience any of these symptoms, particularly sudden onset of floaters, shadows in vision, or vision loss, seeking immediate evaluation by an eye care professional becomes essential. Early detection and appropriate treatment can often prevent additional retinal damage and preserve visual function.
Diagnosis of Ocular Toxoplasmosis
When you present to an eye doctor with symptoms potentially consistent with ocular toxoplasmosis, a comprehensive dilated eye examination becomes necessary. The doctor will instill dilating drops to widen your pupils, allowing thorough visualization of your retina and other internal eye structures. Using specialized magnifying instruments called ophthalmoscopes or slit lamps with additional lenses, the examiner carefully inspects your retinal surface.
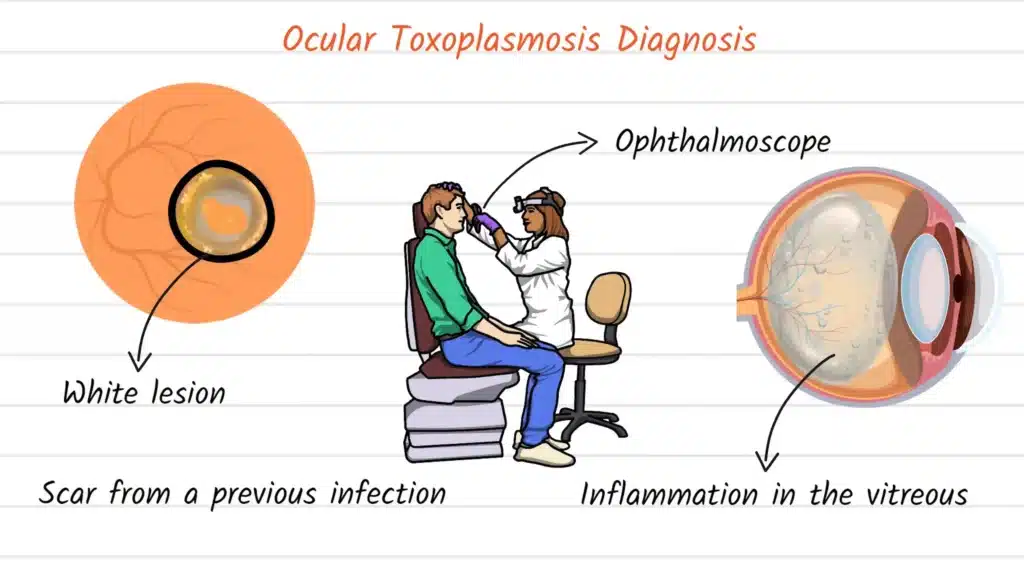
If ocular toxoplasmosis is present, the ophthalmologist will typically observe characteristic findings. Active lesions appear as white or yellowish, fluffy-appearing areas of retinal inflammation. The vitreous humor overlying these lesions often shows inflammatory cells, creating a hazy appearance that ophthalmologists describe as vitritis. Additionally, many patients exhibit old, inactive scars from previous episodes of reactivation, which appear as areas of retinal atrophy with sharp margins and increased pigmentation at their borders.
Blood testing to detect antibodies against Toxoplasma gondii can support the diagnosis, though positive serology simply confirms exposure to the parasite at some point, which is extremely common in the general population. The definitive diagnosis relies primarily on the characteristic appearance of the retinal lesions combined with supporting clinical features and, in many cases, positive serology.
Ocular Toxoplasmosis Treatment
An important point that often surprises patients is that not every case of ocular toxoplasmosis requires immediate treatment. The decision whether to treat depends on several critical factors, including the location of the lesion relative to the macula and optic nerve, the degree of associated inflammation, the current level of visual acuity, and whether the lesion appears active or represents an old, inactive scar.
If a lesion is located peripherally in the retina, far from the macula and optic nerve, and inflammation appears mild, your ophthalmologist might recommend careful observation with periodic monitoring rather than immediate treatment. The rationale behind this conservative approach acknowledges that all antiparasitic medications carry potential side effects, and peripheral lesions that do not threaten central vision may resolve without intervention.
However, when active infection threatens central vision, when inflammation is severe, or when the lesion involves or lies near the macula or optic nerve, treatment becomes necessary. The standard treatment approach combines antiparasitic medications with anti-inflammatory agents. The most commonly utilized antiparasitic combination involves pyrimethamine and sulfadiazine, medications that work synergistically to kill actively replicating parasites.
Because pyrimethamine can interfere with folic acid metabolism and potentially suppress bone marrow function, doctors always prescribe it alongside folinic acid (also called leucovorin) supplementation to prevent these adverse effects. Alternative antibiotic options include azithromycin, trimethoprim-sulfamethoxazole, or clindamycin, which may be selected based on individual patient factors, allergies, or tolerance issues.
In addition to antiparasitic therapy, ophthalmologists typically prescribe corticosteroid medications to reduce inflammation and minimize collateral damage to surrounding healthy retinal tissue. However, corticosteroids are never used alone, as suppressing inflammation without simultaneously killing parasites could theoretically allow unchecked parasite proliferation.
Treatment courses typically extend for four to six weeks, though some cases require longer duration depending on the response observed. Regular follow-up examinations monitor treatment response and allow adjustment of the therapeutic regimen as needed.
The prognosis following treatment generally proves favorable, with most patients experiencing resolution of active inflammation and stabilization of vision. However, some individuals unfortunately experience permanent vision loss, particularly when lesions are large, centrally located, or when treatment begins after significant retinal damage has already occurred.
Potential Complications and Long-Term Considerations
Beyond the direct retinal damage caused by the infection itself, ocular toxoplasmosis can lead to several additional complications. Secondary glaucoma represents one significant concern, as inflammatory cells and debris can obstruct the eye’s internal drainage system, causing increased intraocular pressure that potentially damages the optic nerve. Cataract formation represents another possible complication, particularly in cases with severe, prolonged inflammation or following extended corticosteroid use.
Some patients experience recurrent episodes of reactivation throughout their lives, with each episode carrying risk of additional retinal scarring and progressive vision loss. The factors triggering reactivation remain incompletely understood, though immune system fluctuations clearly play an important role.
Prevention Strategies: Protecting Yourself from Infection
For individuals not yet infected with Toxoplasma gondii, several practical preventive measures can substantially reduce exposure risk. Always cook meat thoroughly to safe internal temperatures, which kills any tissue cysts that might be present. Avoid consuming raw or undercooked meat products, particularly pork, lamb, and venison.
When handling raw meat during food preparation, practice careful hand hygiene, washing thoroughly with soap and water before touching your face or eating. Clean all cutting boards, utensils, and surfaces that contacted raw meat promptly and thoroughly.
If you own cats, particularly outdoor cats with hunting access, take appropriate precautions when handling litter boxes. Ideally, pregnant women and immunocompromised individuals should avoid litter box duties entirely, delegating this task to other household members. When this is not possible, wear disposable gloves, change litter daily (oocysts require 24 hours after shedding to become infectious), and wash hands thoroughly afterward.
During gardening or other soil contact activities, wear gloves and avoid touching your face until after thorough hand washing. Wash all fruits and vegetables carefully before consumption, particularly those that grow close to the ground or might have been exposed to soil contamination.
For individuals already infected but healthy with normal immune function, no treatment is necessary. However, if you become immunocompromised for any reason, discuss your toxoplasmosis status with your healthcare provider, as prophylactic medication might be recommended to prevent reactivation.
Conclusion: Understanding and Managing Ocular Toxoplasmosis
Ocular toxoplasmosis represents a significant cause of vision-threatening posterior uveitis worldwide, affecting millions of individuals. While the prospect of harboring a parasitic infection might seem alarming, understanding that most infected individuals never develop eye problems provides appropriate perspective. For those who do develop ocular manifestations, modern treatment approaches generally prove effective at controlling active disease and preserving vision, particularly when diagnosis occurs promptly and treatment begins before extensive retinal damage accumulates.
The key takeaway involves awareness of symptoms and the importance of prompt evaluation whenever unusual visual symptoms develop. By recognizing potential warning signs like new floaters, shadows in vision, or sudden vision changes and seeking immediate professional assessment, most complications can be prevented or minimized.
Thank you for reading this comprehensive explanation of ocular toxoplasmosis. If you found this information valuable and wish to learn more about various eye diseases and vision health topics, please consider subscribing to our channel and supporting our educational mission. Your engagement helps us continue creating detailed, accessible content to promote eye health awareness and education.
Sources and References
National Center for Biotechnology Information on Ocular Toxoplasmosis (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4850543/)[1]
American Academy of Ophthalmology: Eye Health Information on Ocular Toxoplasmosis (https://www.aao.org/eye-health/diseases/ocular-toxoplasmosis)[2]
National Eye Institute: Eye Conditions and Diseases Resource (https://www.nei.nih.gov/learn-about-eye-health/eye-conditions-and-diseases/ocular-toxoplasmosis)[3]
JAMA Medical Journal: Clinical Research Study on Toxoplasmosis (https://www.jama.com/article.aspx?doi=10.1001/jama.2018.0471)[4]
PubMed Central Research Database: Toxoplasmosis Studies (https://pubmed.ncbi.nlm.nih.gov/28573476/)[5]