Imagine waking up one morning and the left side of the room simply isn’t there — not blurry, not dark, just absent. You reach for your coffee mug and miss it. You walk toward a doorway and clip the frame. Your eyes look completely normal, yet something is clearly wrong.
This is the daily reality for people living with hemianopia, a condition where half of the visual field is lost. It is not a typical eye disease — it is often a signal that something has happened deeper inside the visual system, in the brain itself. Understanding what hemianopia is, why it happens, and how it is managed can make a meaningful difference for patients, families, and caregivers alike.
What Is Hemianopia?
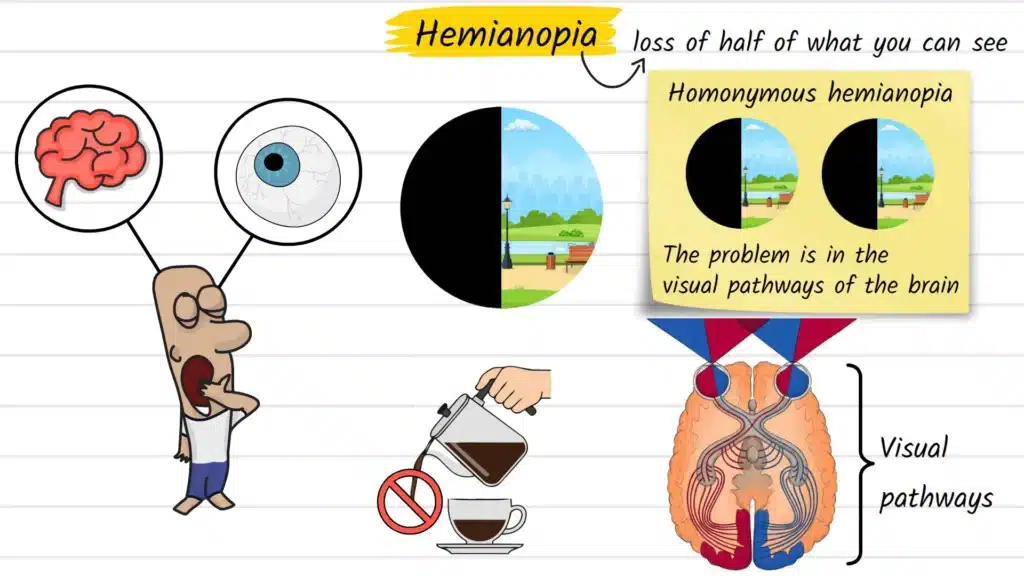
Hemianopia (also spelled hemianopsia) refers to the loss of half of the visual field — the full area you can see when your eyes are focused on a single point. The word comes from Greek: hemi meaning half, and anopia meaning absence of vision.
The most commonly discussed form is homonymous hemianopia, where the same side of vision is missing in both eyes simultaneously. For example, both eyes lose their left visual field — meaning anything on the left side of space goes unnoticed, regardless of which eye is open.
This makes hemianopia fundamentally different from conditions like cataracts or macular degeneration, where the problem is inside the eye itself. In hemianopia, the eyes are often structurally healthy. The disruption occurs along the visual pathways that carry signals from the retina through the brain, particularly in the optic radiations or the visual cortex at the back of the skull.
Causes and Risk Factors
The visual pathway from the eye to the brain is long and vulnerable to a range of neurological events. The most common causes of homonymous hemianopia include:
- Stroke — the leading cause in adults, particularly strokes affecting the occipital lobe or posterior cerebral artery territory
- Traumatic brain injury — vehicle accidents, falls, and sports-related head trauma can all damage visual pathways
- Brain tumors — both primary and metastatic lesions can compress or destroy visual processing areas
- Surgical complications — neurosurgical procedures near the temporal lobe or visual cortex carry a small risk of field loss
- Demyelinating disease — conditions like multiple sclerosis can produce lesions along the optic radiations
- Vascular malformations — arteriovenous malformations or intracranial hemorrhages affecting the posterior brain
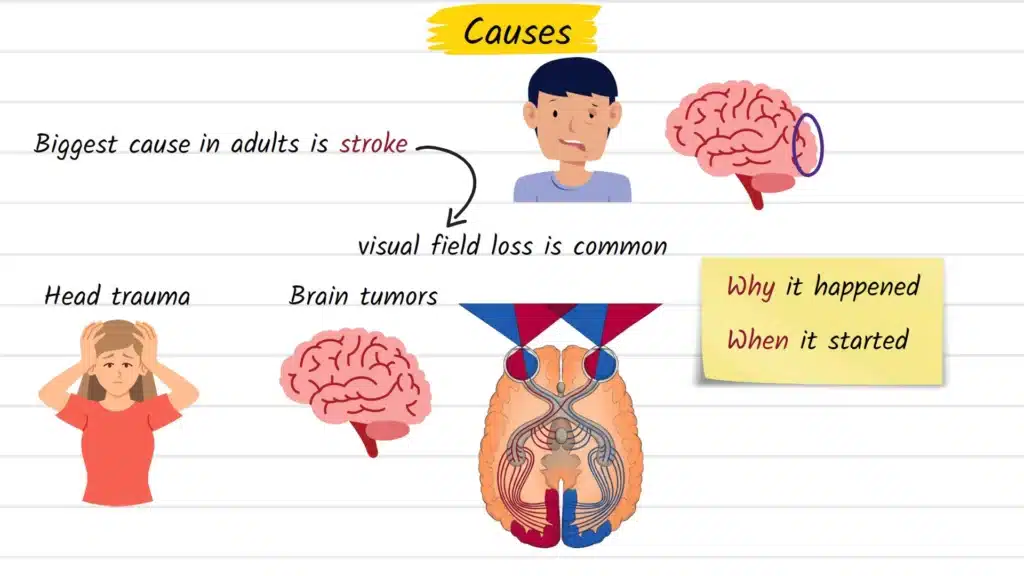
Risk factors largely mirror those for cerebrovascular disease: high blood pressure, diabetes, smoking, cardiovascular disease, older age, and a personal or family history of stroke. A prospective study of stroke patients found that visual field loss is among the most frequently documented neurological consequences following a stroke event.
Common Signs and Symptoms
Hemianopia does not always announce itself dramatically. Many people describe a growing sense of clumsiness or spatial confusion before they identify a visual cause. Common signs include:
- Repeatedly bumping into doorframes, furniture, or people on one side
- Missing food, objects, or text on one side of a surface
- Losing track of words while reading, or consistently skipping to the wrong part of the line
- Difficulty navigating crowded or busy environments
- Near-miss incidents while driving, particularly from hazards on the affected side
- A persistent feeling that “something is off” without being able to explain what
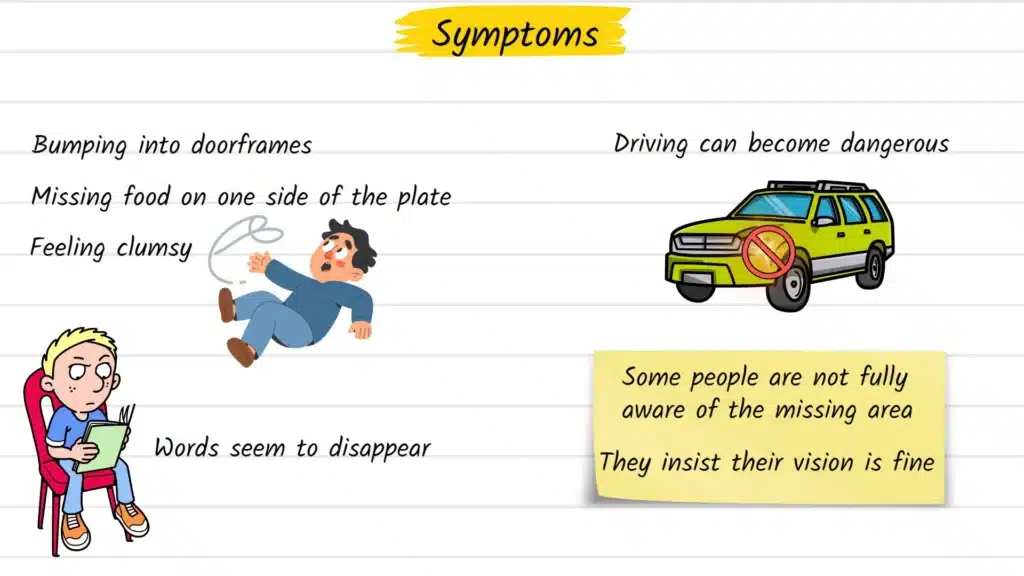
One of the more challenging features of hemianopia is that some patients are not immediately aware of their own visual loss — a phenomenon called anosognosia. These individuals may genuinely believe their vision is intact, even while consistently missing objects on one side. This makes early clinical evaluation — and input from family or caregivers — particularly valuable.
How Hemianopia Is Diagnosed
Diagnosis begins with a detailed clinical history. A clinician will want to know when the change started, whether it came on suddenly or gradually, and whether any other neurological symptoms accompanied it — such as weakness, speech difficulty, headache, or confusion. Sudden onset is treated as a neurological emergency until proven otherwise.
Formal visual field testing (perimetry) is the cornerstone of diagnosis. Using this test, an eye care professional maps exactly which parts of the visual field are intact and which are absent. The precise pattern of loss — which quadrants are affected and whether the defect is symmetric between both eyes — helps pinpoint where along the visual pathway the damage has occurred.
When the pattern suggests a brain-level problem, neuroimaging is the next step. MRI is generally preferred for detecting posterior brain lesions, while CT is commonly used in urgent settings to rule out hemorrhage quickly.
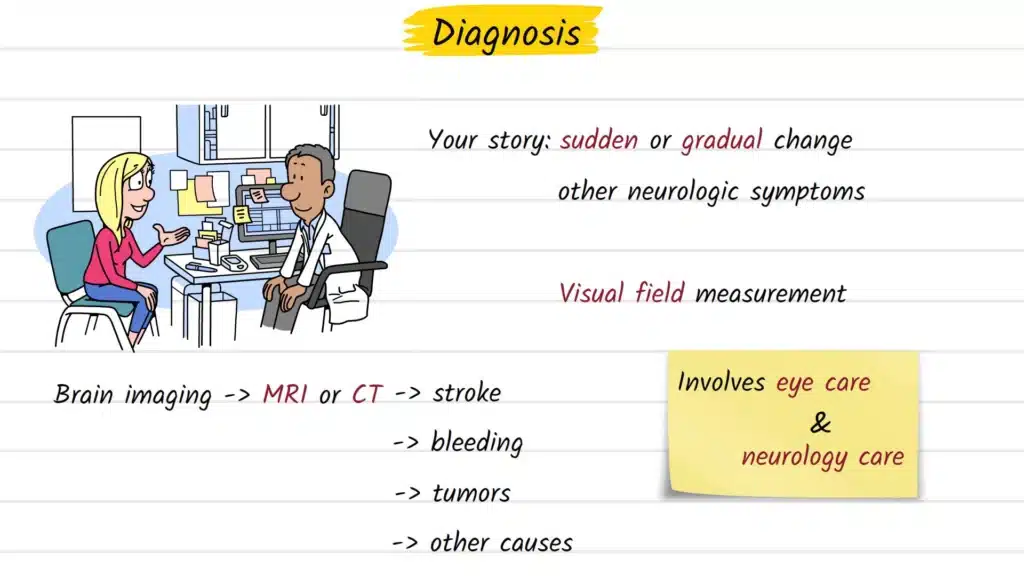
Because hemianopia often implicates both the visual system and the brain, patients are typically managed across specialties — involving ophthalmology or optometry alongside neurology or neuro-ophthalmology.
Treatment Options Explained
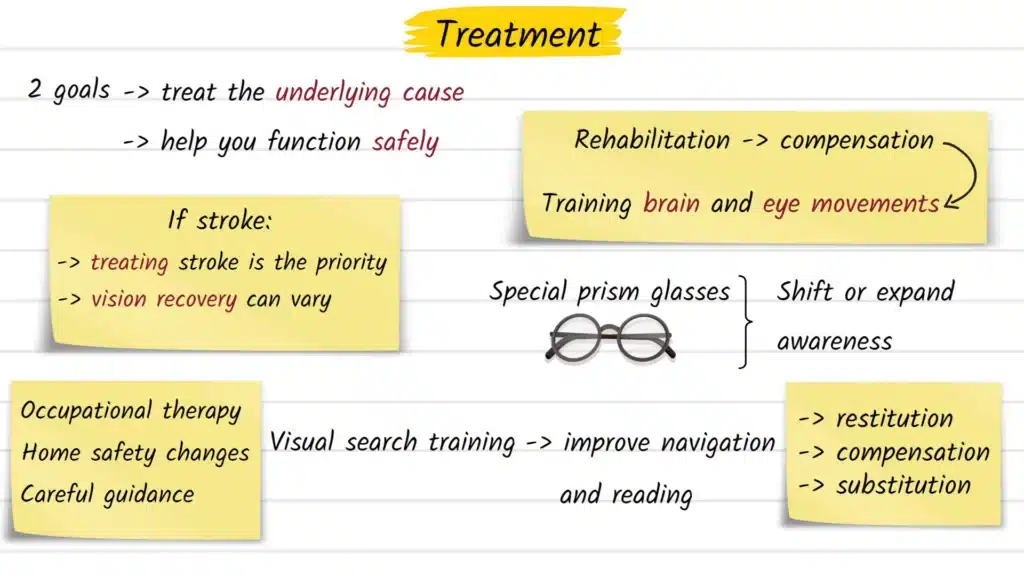
Treatment for hemianopia has two broad goals: addressing the underlying cause, and helping the person function as safely and independently as possible with the vision they have.
Treating the root cause is always the first priority. In stroke, this means acute neurological care, secondary prevention, and structured rehabilitation. In the case of a tumor, surgical, radiation, or oncological management may apply. When the underlying cause is treated promptly, some degree of visual field recovery is possible — though outcomes vary significantly between individuals and cannot be predicted in advance.
Visual rehabilitation takes three general approaches, as outlined in a systematic review published in the Cochrane Database of Systematic Reviews:
- Restitution therapy — intensive stimulation targeting the border zones of the visual field in an attempt to recover lost function; evidence for this approach is still actively being evaluated
- Compensatory training — teaching patients to make deliberate, wider eye movements (saccades) toward the blind side to scan for information they would otherwise miss; this approach has the most consistent clinical support
- Substitution methods — optical aids such as prism glasses, which physically shift or expand awareness toward the affected side, helping with navigation and safety
Reading rehabilitation often requires dedicated attention, as line-by-line reading is heavily disrupted by field loss. Occupational therapy, structured scanning exercises, and assistive technology can all meaningfully improve reading speed and independence.
Practical environmental changes — repositioning commonly used objects, improving room lighting, adjusting kitchen and workspace layouts — frequently produce more immediate functional benefit than people anticipate. Guidance around driving restrictions is also a critical part of safe management.
No single approach works equally well for every patient. A personalized, multidisciplinary plan developed with eye care professionals, neurologists, and occupational therapists is the most effective route forward.
Possible Complications if Left Untreated
Unrecognized or unmanaged hemianopia carries risks beyond the visual field loss itself:
- Road accidents — missing hazards from the blind side makes driving dangerous and is legally restricted in most countries
- Falls and physical injuries — misjudging distances and failing to notice obstacles significantly raises fall risk, particularly in older adults
- Social withdrawal and depression — difficulty navigating public spaces, following visual conversations, and reading independently can lead to isolation and reduced quality of life
- Delayed diagnosis of serious neurological disease — hemianopia can be the first visible symptom of a stroke, tumor, or other urgent brain condition requiring immediate medical attention
Prevention and Risk Reduction
Because most cases of hemianopia result from stroke or brain injury, prevention closely follows standard cerebrovascular risk reduction:
- Keep blood pressure, blood sugar, and cholesterol levels well managed
- Avoid smoking and limit alcohol intake
- Follow a heart-healthy diet and maintain regular physical activity
- Seek immediate medical attention for any symptoms of TIA (transient ischemic attack) or stroke — including sudden visual changes, one-sided weakness, or speech difficulty
- Discuss appropriate preventive medications with your physician if cardiovascular risk factors are present
When to See an Eye Doctor
Any sudden loss or change in visual field should be treated as a medical emergency. Do not wait to see whether it improves on its own.
Seek immediate attention if you experience:
- A sudden loss of half your vision in one or both eyes
- Visual disturbance accompanied by headache, weakness, slurred speech, or confusion
- Any new visual change following a head injury
Schedule a formal evaluation if you notice:
- Repeatedly bumping into things on one specific side
- Consistently missing words or lines while reading
- Unexplained spatial clumsiness in familiar environments
Early evaluation by an eye care professional can not only clarify the nature of the visual loss but also trigger the neurological investigation needed to identify and treat the underlying cause.
Frequently Asked Questions
Hemianopia is the loss of half the visual field, not complete vision loss. Both eyes may remain structurally healthy. The problem lies in the brain’s visual processing pathways rather than the eyes themselves.
Some recovery is possible, particularly in the weeks immediately following a stroke, as swelling decreases and the brain begins to adapt. However, complete spontaneous recovery is uncommon. Rehabilitation significantly improves functional outcomes even when the field loss itself remains.
In homonymous hemianopia, the same side of the visual field is lost in both eyes. This happens because the visual pathways for both eyes merge and travel together through the brain from the optic chiasm onward.
In most countries, hemianopia is a disqualifying condition for driving without formal re-assessment. A specialist driving evaluation is typically required before any return to driving is considered, if it is permitted at all.
Management usually involves a multidisciplinary team that may include a neurologist, neuro-ophthalmologist, optometrist, and occupational therapist, depending on the underlying cause and rehabilitation needs.
Prism lenses can benefit some patients by shifting visual awareness toward the affected side. They are not universally appropriate and should be evaluated and fitted by a specialist with experience in low vision rehabilitation.
No. Tunnel vision (concentric field loss) involves the progressive narrowing of the visual field from the outer edges inward. Hemianopia involves the loss of one specific half of the visual field, typically as a result of a distinct neurological event.
Sources and Further Reading
- Goodwin D. Homonymous hemianopia: challenges and solutions. Clinical Ophthalmology, 2014. Read on PubMed Central
- Rowe FJ et al. Visual effects and rehabilitation after stroke. Future Neurology, 2017. Read on PubMed Central
- Rowe FJ et al. Interventions for visual field defects in people with stroke. Cochrane Database of Systematic Reviews. View on Wiley
- Gilhotra JS et al. A Prospective Profile of Visual Field Loss following Stroke. BioMed Research International, 2013. View article
Educational Disclaimer
This article is intended for general informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified eye care professional or physician regarding any concerns about your vision or neurological health. If you are experiencing a sudden change in vision, seek emergency medical care immediately.