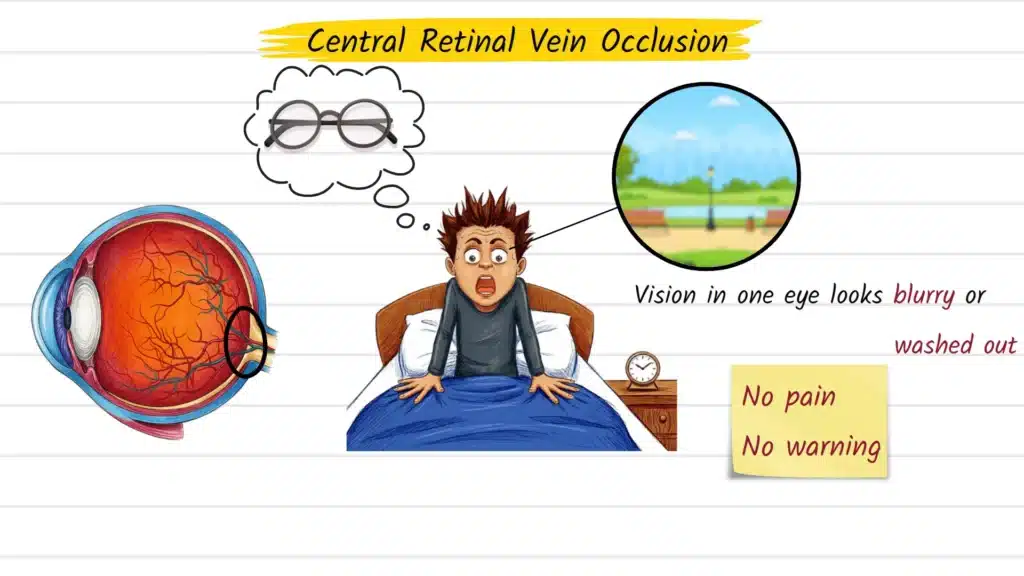
You wake up one morning and something looks different in one eye — a haziness that won’t clear, a patch of blurred vision, or a subtle darkening that wasn’t there the day before. No pain, no obvious warning sign. It would be easy to assume you need a new glasses prescription or slept in an awkward position.
But sudden, painless vision changes in a single eye are one of the most important signals the eye can send. Central retinal vein occlusion (CRVO) is a serious retinal condition that fits exactly this pattern, and understanding it — what it is, why it happens, and when to seek care — can genuinely affect the outcome.
What Is Central Retinal Vein Occlusion?
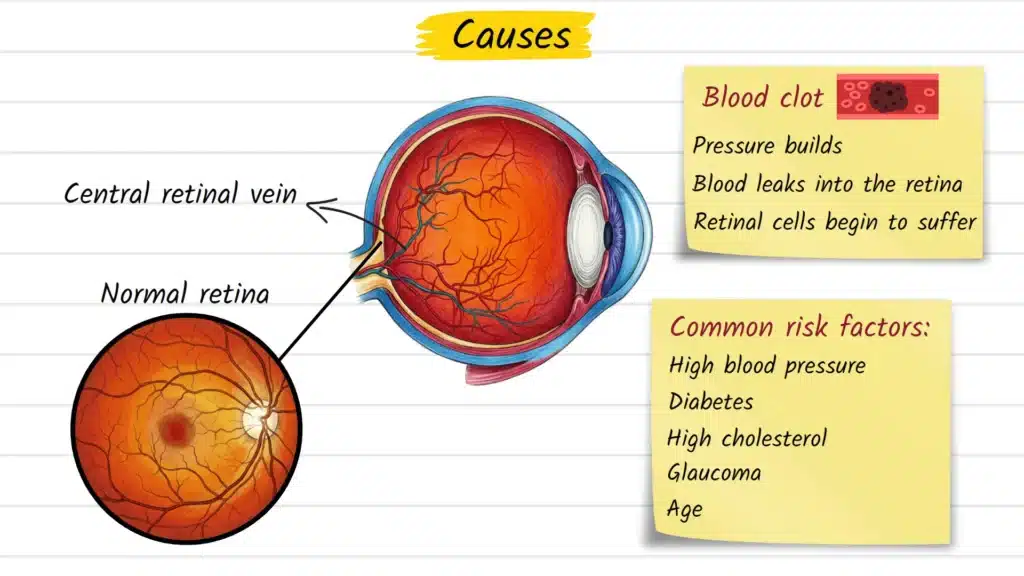
Central retinal vein occlusion (CRVO) is a blockage of the central retinal vein, the primary vessel responsible for draining blood away from the retina. The retina is the thin, light-sensitive layer lining the back of the eye that converts visual information into signals travelling to the brain.
When this drainage pathway becomes obstructed — most often by a blood clot — pressure builds within the smaller retinal vessels. Blood and fluid leak into retinal tissue, cells begin to suffer from reduced oxygen supply, and vision in the affected eye deteriorates. The pattern of damage that results is clinically distinctive and often described as looking like a storm passed through the inside of the eye.
CRVO affects the entire retina because it involves the main central vein. This sets it apart from branch retinal vein occlusion (BRVO), where only a smaller tributary is blocked and damage is more localised.
Causes and Risk Factors
CRVO rarely occurs in isolation — it is frequently the eye’s signal that something systemic is affecting the cardiovascular or circulatory system. The blockage itself usually results from one or more of three mechanisms: narrowing of the vein wall, blood with an increased tendency to clot, or compression of the vein by an adjacent artery where the two share a common tissue sheath near the optic nerve head.
The most well-established risk factors include:
- High blood pressure (hypertension) — the single most common systemic contributor
- Diabetes mellitus, particularly with poor long-term blood sugar control
- Elevated cholesterol (hyperlipidaemia)
- Glaucoma — raised intraocular pressure independently increases CRVO risk
- Age over 50 — prevalence rises significantly in older adults
- Cardiovascular disease, including a history of heart attack or stroke
- Obesity and physical inactivity
- Smoking
- Blood clotting disorders (thrombophilia) — more relevant in younger patients without obvious vascular risk factors
In younger individuals presenting without typical cardiovascular risk factors, clinicians often investigate for underlying clotting disorders, autoimmune conditions, or inflammatory causes.
Common Signs and Symptoms
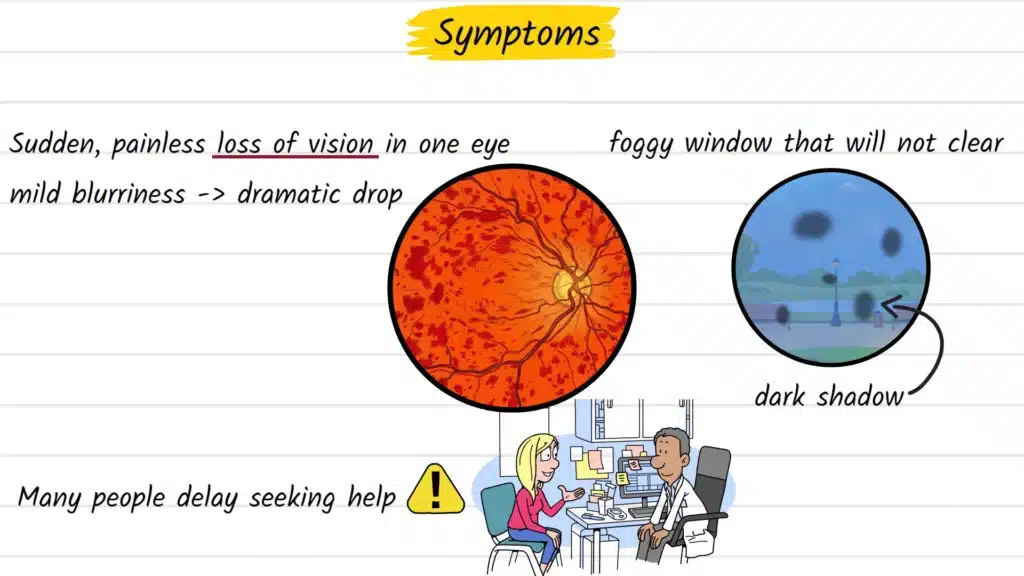
The defining feature of CRVO is a sudden, painless change in vision confined to one eye. The complete absence of pain is precisely why many people delay seeking care, reasoning that a painless problem is probably not urgent. In retinal vascular conditions, this assumption can be costly.
Symptoms vary depending on how severely the macula — the small central region of the retina responsible for sharp, detailed vision — is involved:
- Blurring or haziness in one eye, as though looking through a frosted window
- A rapid drop in visual clarity or sharpness
- A dark shadow or grey patch obscuring part of the visual field
- Distortion of straight lines (a symptom called metamorphopsia, typically indicating macular involvement)
- Reduced contrast sensitivity or colour perception
Bilateral, simultaneous vision changes point toward different diagnoses. CRVO is a one-eye condition.
How Central Retinal Vein Occlusion Is Diagnosed
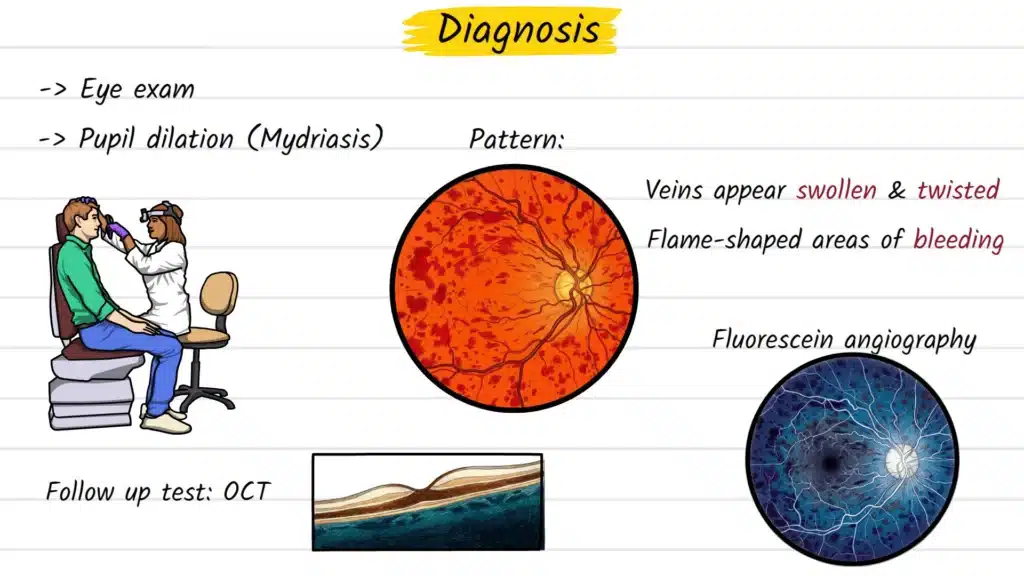
Diagnosis begins with a comprehensive dilated fundus examination. The clinician instils drops to temporarily widen the pupil, enabling a clear view of the posterior pole. In CRVO, the retinal appearance is quite characteristic: tortuous, engorged veins spanning all four retinal quadrants, flame-shaped haemorrhages distributed throughout, and often swelling at the optic disc. The appearance is sometimes referred to as a “blood and thunder fundus” in clinical teaching.
Several imaging modalities are typically used alongside clinical examination:
- Optical Coherence Tomography (OCT): A non-invasive, high-resolution retinal scan. Critically useful for detecting and measuring macular oedema — the fluid accumulation in the central retina that is the primary driver of vision loss in CRVO.
- Fluorescein Angiography (FA): A contrast dye is injected intravenously and retinal photographs are taken as it circulates, identifying areas of non-perfusion, leakage, and the extent of ischaemia.
- OCT Angiography (OCTA): A newer, dye-free technique that maps retinal blood flow and can detect capillary dropout without the need for injection.
Systemic investigation is standard practice following a CRVO diagnosis — including blood pressure measurement, fasting glucose, and a full lipid panel. In younger patients or atypical presentations, a thrombophilia screen and inflammatory markers may be added.
Treatment Options Explained
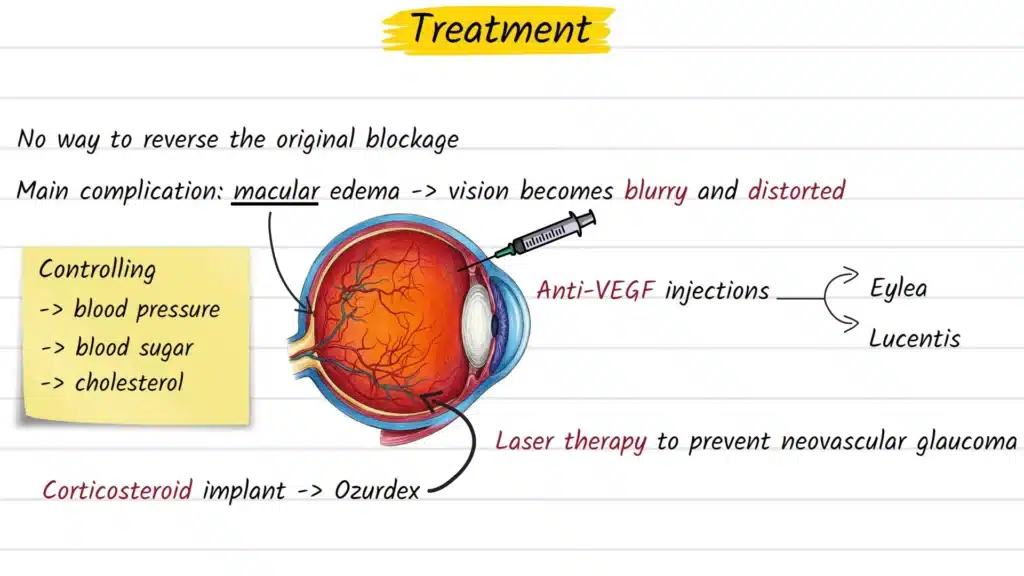
There is currently no treatment that reverses the original venous occlusion once it has occurred. What can be treated, effectively and with well-documented results, is the most vision-threatening complication that follows: macular oedema.
Anti-VEGF Intravitreal Injections
The current first-line treatment for CRVO-associated macular oedema is intravitreal anti-VEGF therapy. These injections are administered directly into the vitreous cavity of the eye — a procedure performed under topical anaesthesia in a clinical setting. Agents such as ranibizumab, aflibercept, and bevacizumab block vascular endothelial growth factor (VEGF), a protein that drives fluid leakage and the growth of abnormal blood vessels. Multiple injections over time are generally required, and evidence from large-scale clinical trials supports meaningful visual improvement in a substantial proportion of patients.
Intravitreal Corticosteroid Implants
A slow-release dexamethasone implant (Ozurdex) is an alternative for patients who respond inadequately to anti-VEGF therapy or in specific clinical circumstances. It delivers controlled steroid therapy over several months. Monitoring for raised intraocular pressure and accelerated cataract development is important with this option.
Laser Photocoagulation
When retinal ischaemia is extensive, areas of oxygen-deprived tissue can trigger the growth of fragile new blood vessels — a process called neovascularisation. Pan-retinal photocoagulation (PRP) is used to prevent the potentially severe complication of neovascular glaucoma. Laser treatment in this context is preventive rather than vision-restoring.
Systemic Risk Factor Control
Managing blood pressure, blood sugar, and cholesterol is not a secondary concern — it is fundamental to long-term outcomes and to reducing the risk of a repeat occlusive event. Collaboration between the eye specialist and the patient’s general practitioner or internist is strongly recommended as part of ongoing care.
Possible Complications if Left Untreated
Without timely diagnosis and management, CRVO can lead to:
- Persistent macular oedema causing permanent central vision loss
- Progressive retinal ischaemia as more capillaries lose function
- Neovascularisation on the retinal surface, iris, or drainage angle of the eye
- Neovascular glaucoma — a severe condition in which new blood vessels obstruct the eye’s drainage system, causing dangerously elevated intraocular pressure
- Vitreous haemorrhage from rupture of fragile new vessels
The severity of these complications depends largely on the degree of retinal ischaemia and the speed at which treatment is initiated.
Prevention and Risk Reduction
While CRVO cannot always be prevented, protecting cardiovascular health addresses the core underlying risk:
- Keep blood pressure well-controlled through lifestyle modifications and, where appropriate, medication
- Maintain stable blood sugar levels if you have diabetes
- Manage cholesterol through diet, physical activity, and prescribed therapy where indicated
- Stop smoking — it is an independent vascular risk factor
- Exercise regularly and maintain a healthy body weight
- Attend routine eye examinations, especially from age 40 onwards — glaucoma and early hypertensive retinal changes can be identified before complications develop
For individuals who have already experienced a CRVO, regular follow-up and systemic evaluation are standard. The risk of further vascular events — whether in the fellow eye or elsewhere — warrants ongoing monitoring.
When to See an Eye Doctor
Seek an urgent eye examination — ideally within 24 to 48 hours — if you notice any of the following in one eye:
- A sudden change in vision that appears without pain or obvious cause
- A new shadow, curtain, or dark patch anywhere in your visual field
- Blurring that develops quickly and does not resolve
- Distortion or waviness in straight lines you previously saw clearly
Do not wait to see whether symptoms improve on their own. In retinal vascular conditions, early assessment is one of the most significant factors influencing how much vision can ultimately be preserved.
Frequently Asked Questions
High blood pressure is the most common systemic cause. CRVO occurs when the central retinal vein becomes blocked — most often by a thrombus — disrupting normal blood drainage from the retina. Conditions that damage blood vessel walls or alter clotting behaviour are the primary contributors.
The original blockage cannot be reversed once it has occurred. However, the main vision-threatening complication — macular oedema — can be treated effectively with anti-VEGF injections or corticosteroid implants, and many patients experience significant visual improvement with timely care.
CRVO and stroke share overlapping risk factors, including hypertension, diabetes, and cardiovascular disease. A CRVO diagnosis should prompt thorough systemic evaluation. However, CRVO does not directly cause stroke — it is a localised vascular event in the eye.
Recovery varies considerably between patients. Some regain substantial vision with treatment, while others — particularly those with extensive retinal ischaemia — may have lasting changes. Most treatment programmes involve regular clinic visits over 12 to 24 months.
No — these are separate conditions. CRVO involves a blocked blood vessel causing bleeding and swelling within the retina. Retinal detachment involves the retinal tissue physically separating from the supportive layer beneath it. Both are serious and require urgent assessment, but their causes, appearance, and management are different.
Bilateral simultaneous CRVO is uncommon. When it occurs, it often prompts investigation for an underlying systemic clotting disorder or other contributory cause.
Persistent macular oedema can cause progressive and potentially irreversible damage to the photoreceptors responsible for central and fine-detail vision. Early, consistent treatment substantially reduces this risk.
References and Further Reading
- Rehak, M. & Wiedemann, P. (2010). Retinal vein thrombosis: pathogenesis and management. Journal of Thrombosis and Haemostasis. Read on PMC
- Scott, I.U., et al. (2020). Retinal vascular occlusions. The Lancet. Read on PMC
- Royal College of Ophthalmologists (2022). Retinal Vein Occlusion Guidelines. Eye. Read on PMC
- Kido, A., et al. (2022). Risk Factors and Treatment Strategy for Retinal Vascular Occlusive Diseases. Journal of Clinical Medicine. Read on PMC
- American Academy of Ophthalmology. Retinal Vein Occlusions: Preferred Practice Pattern. View on AAO.org