Key Takeaways
- A choroidal nevus is a benign pigmented lesion in the choroid, essentially a mole inside the eye
- It is common, often found incidentally during dilated eye exams, and usually causes no symptoms
- A small number can transform into choroidal melanoma, making monitoring essential
- Risk is assessed using the TFSOM-DIM criteria; more risk features means closer follow-up
- Management for low-risk nevi is observation with structured imaging, not treatment
- Any new visual symptoms in a person with a known nevus warrant prompt evaluation
Picture this: you go in for a routine eye exam, your vision seems fine, and your eye doctor mentions they spotted a small pigmented lesion at the back of your eye. Before you start worrying, know this: what they found is likely a choroidal nevus, and for most people, it is completely harmless.
Still, the word “tumor” appearing in an eye report understandably raises questions. This article explains what a choroidal nevus is, what causes it, how doctors monitor it, and most importantly what warning signs should prompt a closer look.
What Is a Choroidal Nevus?
A choroidal nevus is a flat, pigmented lesion located in the choroid, the thin layer of blood vessels that sits just beneath the retina at the back of the eye. Think of it as a birthmark or a mole, except it forms inside the eye rather than on the skin.
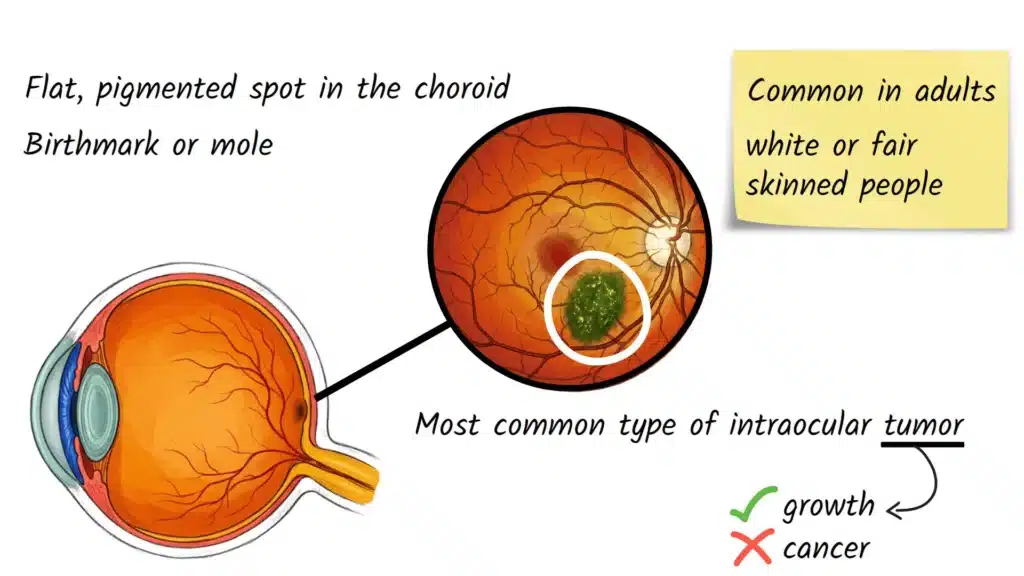
It is the most common type of intraocular tumor found in adults, but the word “tumor” here simply refers to an abnormal growth of cells, not necessarily cancer. The vast majority of choroidal nevi are benign and never cause problems. What makes eye doctors pay attention is that a small number can, over time, slowly transform into a malignant tumor called choroidal melanoma, which is why proper documentation and monitoring matter.
Causes and Risk Factors
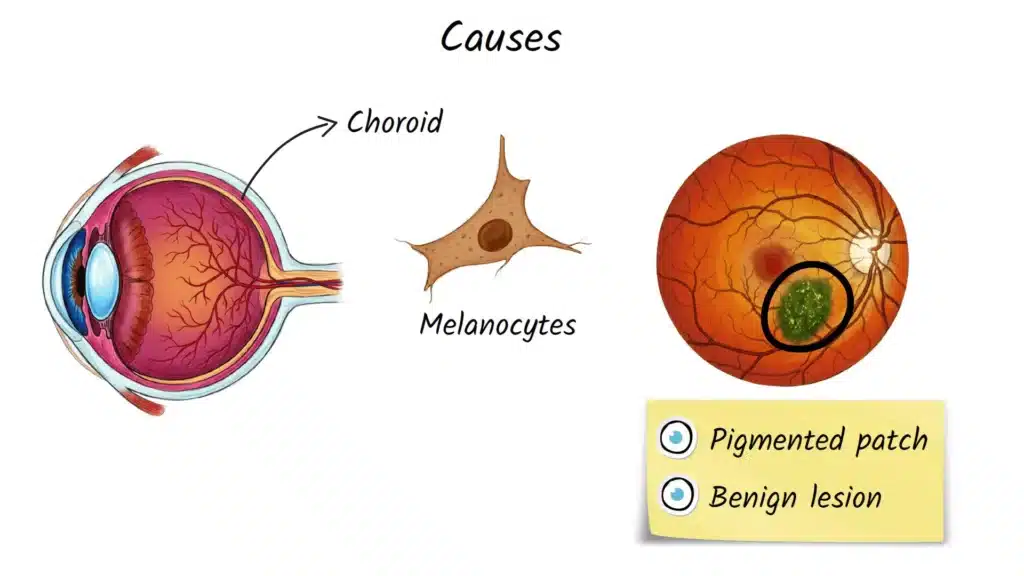
A choroidal nevus forms when melanocytes, the pigment-producing cells inside the choroid, multiply in a localized area, creating a flat or very slightly raised patch of pigmentation. Exactly why this happens in some people and not others is not fully understood, but certain patterns have emerged from research.
Key observations include:
- More commonly found in adults and fair-skinned or light-eyed individuals
- Thought to arise from the same type of cells responsible for skin moles
- Not caused by eye strain, screen time, or sunlight exposure directly to the back of the eye
- Not considered hereditary in the typical sense, though melanocyte biology plays a role
Beyond the presence of a nevus itself, clinicians focus on specific features that suggest higher risk of transformation into melanoma. A widely used clinical mnemonic, TFSOM-DIM, helps organize these risk factors:
- T — Thickness greater than 2 mm
- F — Subretinal fluid present
- S — Symptoms such as blurred vision
- O — Orange pigment (lipofuscin) visible over the lesion
- M — Melanoma-like hollowness on ultrasound
- DIM — Diameter greater than 5 mm
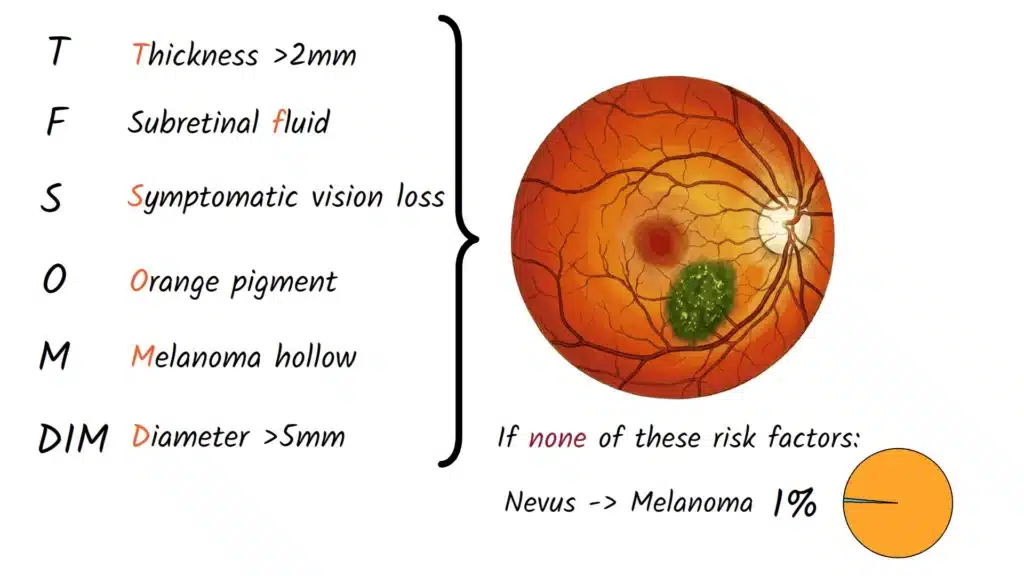
Research published by Shields et al. has shown that a nevus with none of these features carries roughly a 1% risk of transforming into melanoma over five years. Each additional risk factor meaningfully increases that probability, which is why thorough documentation at the first visit is so important.
Common Signs and Symptoms
Most people with a choroidal nevus have absolutely no symptoms. That is precisely why these lesions are so often discovered by surprise during a routine dilated eye exam, the patient feels fine, and the doctor notices it while examining the retina.
When symptoms do occur, they usually arise because the nevus is affecting the retina directly above it. Possible symptoms include:
- Blurred or distorted central vision in one eye
- A gray, dark, or shadowy spot in the visual field
- Straight lines appearing wavy or bent (metamorphopsia)
- Letters or words appearing faded or missing in one part of the visual field
- Reduced vision that does not improve with a new glasses or contact lens prescription
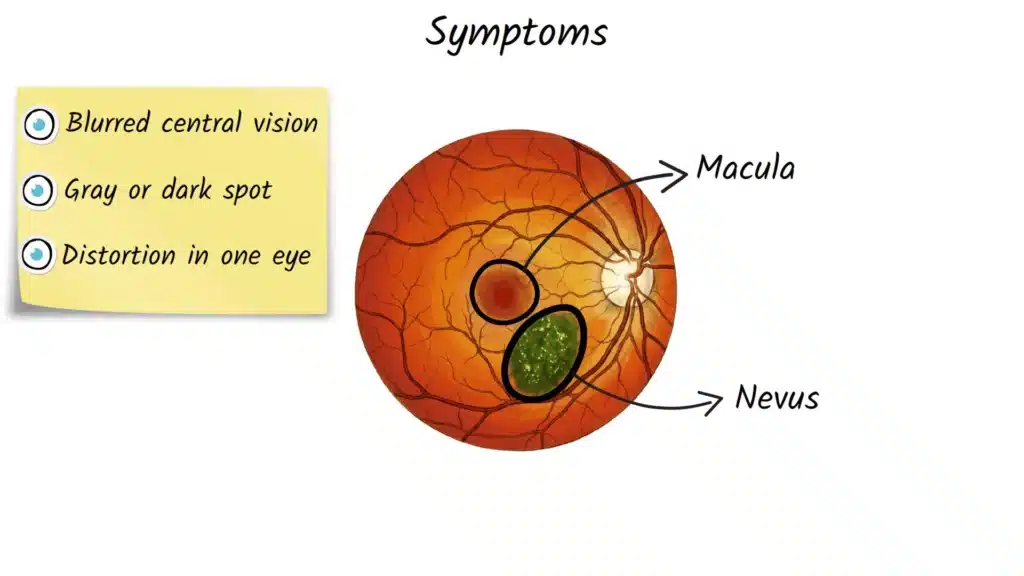
These symptoms are most likely when the nevus sits beneath or near the macula, the part of the retina responsible for sharp, central vision or when it causes fluid to accumulate under the retinal surface. The nevus itself is not painful.
How the Condition Is Diagnosed
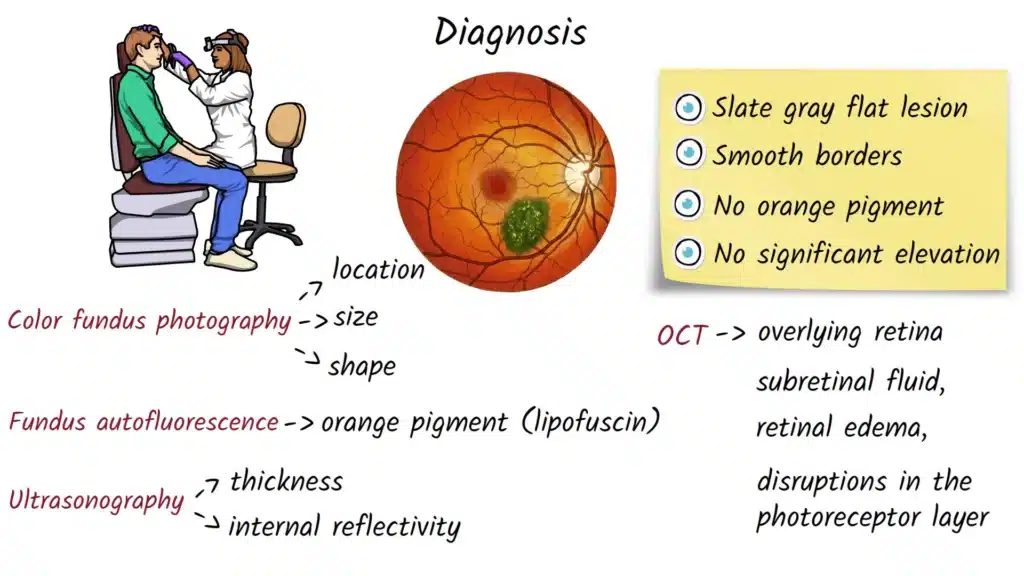
Diagnosis starts with a dilated fundus examination, where the eye doctor uses special lenses and a bright light to examine the back of the eye directly. A typical low-risk nevus appears as a flat, slate-gray or brownish lesion with smooth, well-defined borders, no orange tint, and no elevation.
Modern practice, however, relies on multimodal imaging to document the lesion accurately and detect any changes over time:
- Color fundus photography: Captures the location, size, shape, and pigmentation of the lesion, serving as the baseline for all future comparisons
- Optical coherence tomography (OCT): Shows cross-sectional detail of the retina above the nevus, revealing subretinal fluid, retinal swelling, or photoreceptor disruption that can explain visual symptoms
- Fundus autofluorescence (FAF): Highlights orange pigment (lipofuscin) over the lesion, which is a recognized risk feature
- B-scan ultrasonography: Measures the physical thickness of the lesion and evaluates its internal structure; a benign nevus typically shows high internal reflectivity, while melanoma often shows acoustic hollowing
Together, these tools allow clinicians to classify a lesion as low-risk or suspicious and to establish an appropriate follow-up schedule.
Treatment Options Explained
The good news is that most choroidal nevi require no active treatment. The standard management for a stable, low-risk lesion is watchful waiting with structured monitoring, baseline imaging at the first visit, a follow-up exam within a few months, and then, if the lesion remains stable, periodic check-ins extending to annual or biennial intervals.
If a nevus begins showing growth or accumulates multiple TFSOM-DIM risk features, it is no longer managed as a simple benign lesion. At that stage, referral to an ocular oncology specialist or retina specialist is appropriate for further evaluation.
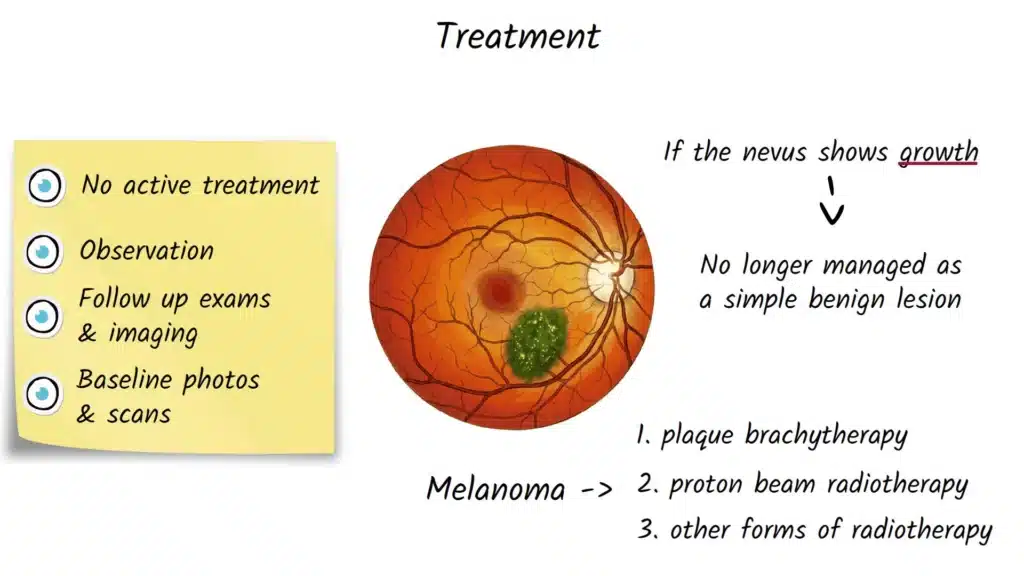
For lesions that have transformed into small choroidal melanoma, treatment options discussed in the literature include:
- Plaque brachytherapy: A small radioactive disc placed on the outer wall of the eye to deliver targeted radiation
- Proton beam radiotherapy: External radiation precisely aimed at the lesion
- Other forms of radiotherapy: Designed to control tumor growth while preserving as much vision as possible
These decisions are made by specialized teams and go well beyond routine optometric or general ophthalmologic care. The primary role in most clinical settings is accurate documentation, recognition of change, and timely referral.
Possible Complications if Left Untreated
A truly stable, low-risk nevus monitored regularly is unlikely to cause harm. However, failing to monitor a nevus or dismissing new symptoms carries real risks:
- Delayed diagnosis of choroidal melanoma, which can metastasize (most commonly to the liver) if not caught early
- Chronic subretinal fluid causing progressive, sometimes irreversible central vision loss
- Photoreceptor damage in the macula from prolonged fluid accumulation
- Missed growth, since small melanomas may be clinically indistinguishable from suspicious nevi without regular imaging
This is why consistent follow-up, even for lesions initially classified as benign, remains the cornerstone of safe management.
Prevention and Risk Reduction
There is currently no known way to prevent a choroidal nevus from forming. However, several steps can support early detection and reduce the chance of complications going unnoticed:
- Attend regular dilated eye exams, especially after age 40
- Report any unexplained change in vision, particularly in one eye, to your eye doctor promptly
- Ensure your eye doctor is aware of your history if a nevus has been documented previously
- If you are fair-skinned with light eyes, mention this context since it is associated with higher prevalence
When to See an Eye Doctor
You should contact your eye doctor promptly if you experience:
- Sudden blurred or distorted vision in one eye
- A new shadow, blind spot, or dark area in your vision
- Straight lines appearing wavy when they should be straight
- Any unexplained visual change that does not resolve within a day or two
If you have already been told you have a choroidal nevus and you experience any of these changes between scheduled visits, do not wait for your next appointment, call your provider.
Frequently Asked Questions
Most choroidal nevi are benign and never cause problems. However, a small percentage can transform into choroidal melanoma over time, which is why regular monitoring with imaging is recommended even for low-risk lesions.
Choroidal nevi are the most common intraocular tumors in adults. They are found more frequently in fair-skinned populations and become more prevalent with age.
Most people with a choroidal nevus have normal vision and no symptoms. Vision problems can occur if the nevus is located near the macula or causes fluid to accumulate under the retina.
Doctors use a combination of clinical examination and imaging — including fundus photography, OCT, autofluorescence, and ultrasound — to evaluate size, thickness, the presence of orange pigment, and subretinal fluid. These findings are assessed against established risk criteria such as the TFSOM-DIM mnemonic.
This depends on its risk profile. A low-risk, stable nevus may only need annual or biennial imaging after initial documentation. A lesion with suspicious features requires more frequent evaluation and possible referral to an ocular oncology specialist.
The vast majority of nevi do not require any treatment. Intervention is only considered if the lesion grows or shows features consistent with melanomatous transformation.
This question applies to lesions that have been treated as melanoma. Recurrence risk and management depend on the individual case and are best discussed with an ocular oncologist.
References and Further Reading
- Shields CL, et al. Understanding Choroidal Nevus Risk Factors for Transformation into Melanoma — Clinics in Dermatology, 2023
- Shields CL, et al. White Paper on Ophthalmic Imaging for Choroidal Nevus Identification and Transformation into Melanoma — PMC / American Journal of Ophthalmology, 2021
- Say EA, et al. Optical Coherence Tomography of Retinal and Choroidal Tumors — PMC, 2011
- Malignant Transformation of a Choroidal Nevus — Case-Based Review — PMC, 2024
- Large Choroidal Nevus vs. Small Choroidal Melanoma — Classification Discussion — PMC, 2021
- Choroidal Nevus Features Associated with Subspecialty Referral — PMC, 2024
Medical Disclaimer
This article is intended for educational and informational purposes only. It does not constitute medical advice and should not be used as a substitute for professional diagnosis or treatment. If you have concerns about your eye health, please consult a qualified eye care provider.
About the Author
This article was written and reviewed by a professional with a background in optometry and ophthalmic education, with a focus on making complex eye conditions accessible to patients and students alike.