Endophthalmitis is a serious infection inside the eye and is treated as a medical emergency because delays can raise the risk of permanent vision loss. It matters because infection and inflammation inside the eye can damage delicate structures quickly, especially the vitreous and retina.
Endophthalmitis is uncommon, but when it happens, fast recognition is critical. It most often follows eye surgery or eye injury, although in some cases the infection reaches the eye through the bloodstream from another part of the body.
What is Endophthalmitis?
Endophthalmitis is an infection and severe inflammation inside the eye, usually involving the fluids and tissues in the front and back of the eye. In practical terms, it is not the same as a routine irritated red eye after a procedure; it is a deep intraocular infection that needs urgent ophthalmic assessment.
Doctors often divide endophthalmitis into two main types.
- Exogenous endophthalmitis: germs enter the eye directly, usually after surgery, an intravitreal injection, or penetrating trauma.
- Endogenous endophthalmitis: germs spread to the eye through the bloodstream from an infection elsewhere in the body.
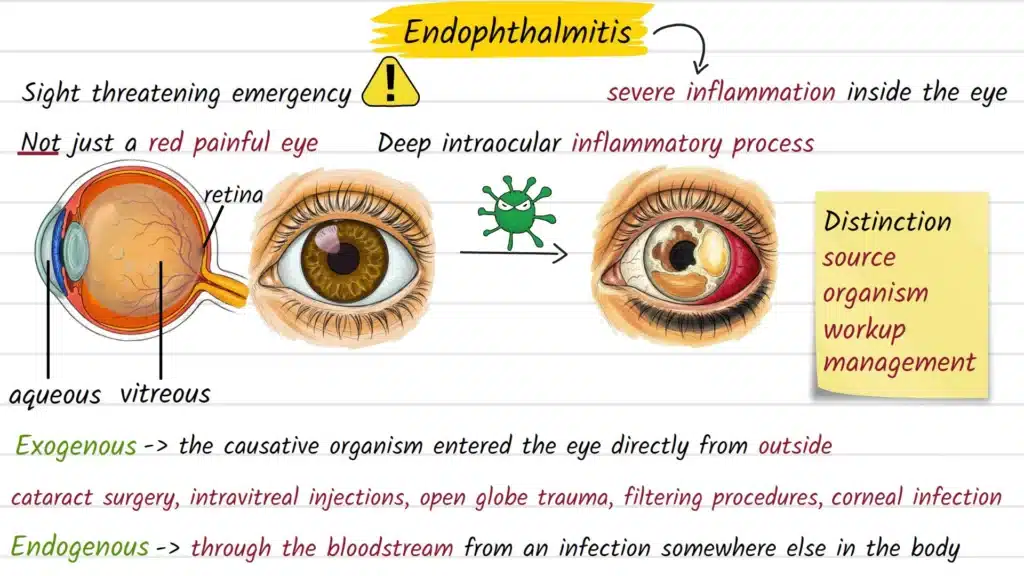
This distinction matters because the likely source, likely organism, and broader medical workup can differ.
Causes and Risk Factors
The most common causes depend on the clinical setting. Exogenous cases usually happen after intraocular surgery, following an eye injury, or less commonly after direct spread from infection near the eye.
Postoperative endophthalmitis is especially important because it can occur after commonly performed procedures, including cataract surgery. Trauma-related cases are often more dangerous when foreign material remains in the eye or when soil and environmental contamination are involved.
Endogenous endophthalmitis begins differently. Instead of entering from outside, organisms travel in the blood and seed the eye from another infection source.
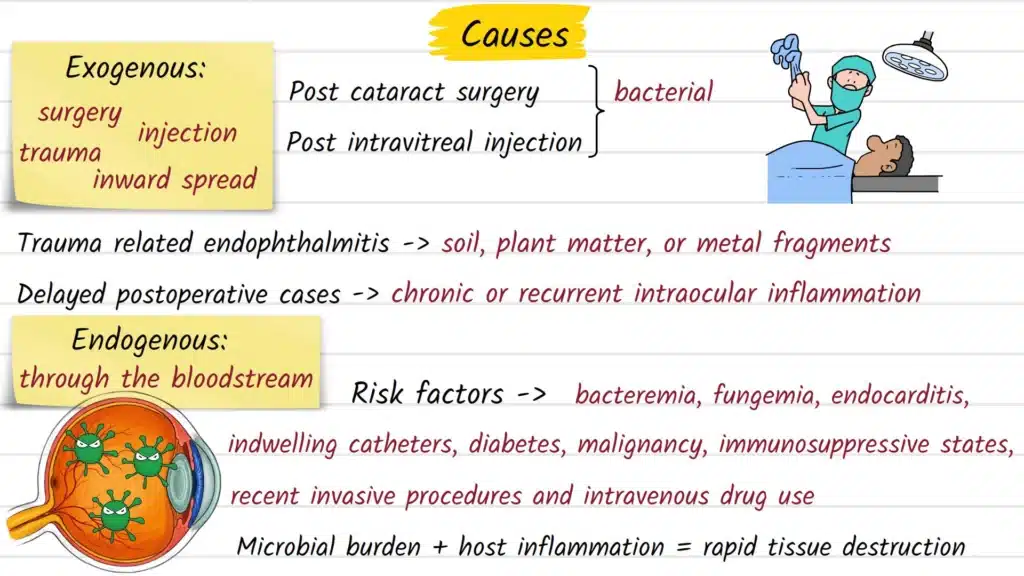
Risk factors described by major ophthalmic references include:
- Recent eye surgery or an intravitreal injection.
- Penetrating eye trauma.
- Retained intraocular foreign body after injury.
- Delayed repair of a full-thickness eye laceration.
- Bloodstream infection, sepsis, or infection after invasive procedures elsewhere in the body.
- Weakened immune system or serious systemic illness.
Although bacteria cause many cases, fungi and other organisms can also be responsible, especially in endogenous disease.
Common Signs and Symptoms
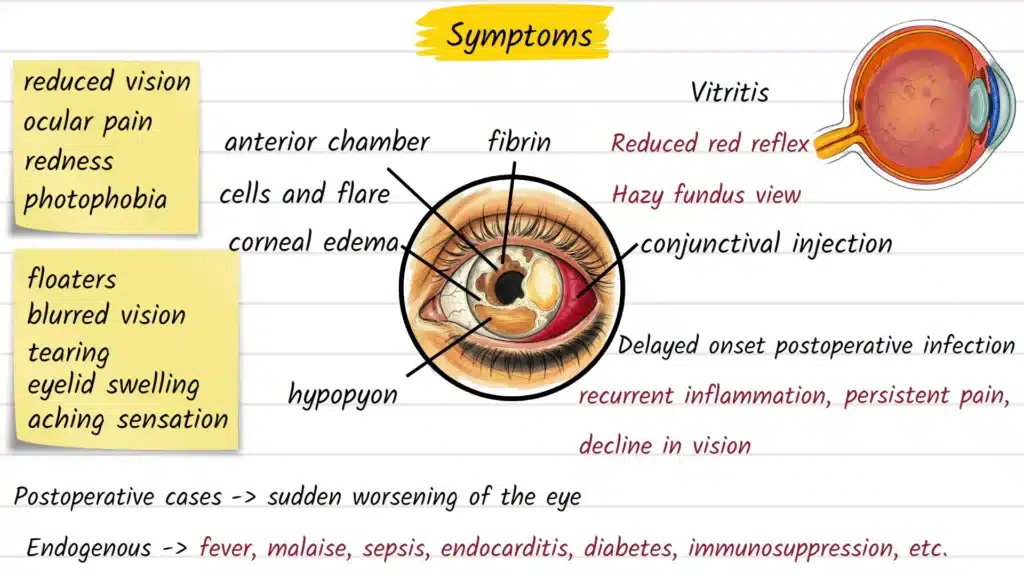
The most common symptoms are eye pain, redness, and reduced vision. Many people also develop marked light sensitivity, sometimes along with eyelid swelling or a sense that the eye is suddenly worsening instead of recovering.
Clinical references describe several warning signs that should raise concern:
- Sudden or progressive blurred vision.
- Severe eye pain.
- Redness of the eye.
- Photophobia, or discomfort in bright light.
- Swelling of the eyelid in some cases.
- A visible layer of inflammatory material in the front of the eye, called a hypopyon.
A particularly important clue is a patient who seems to be recovering after surgery and then suddenly becomes worse over hours or days. In endogenous disease, the eye symptoms may appear alongside signs of systemic infection rather than in isolation.
How the Condition is Diagnosed
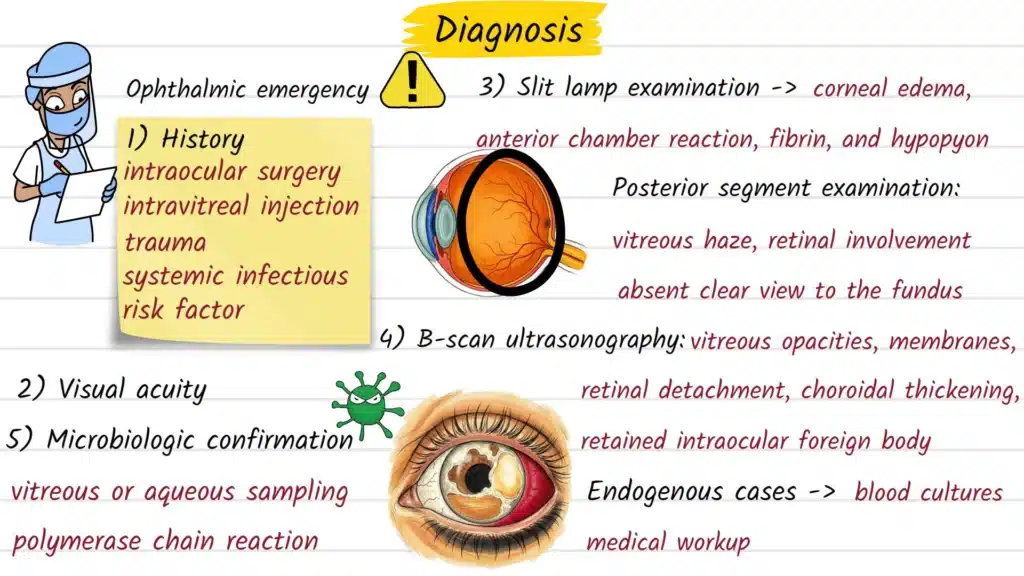
Diagnosis is based on urgent clinical examination by an eye specialist, supported by testing to identify the organism. Doctors assess symptoms, examine the eye, and usually obtain samples of fluid from the front of the eye or the vitreous for laboratory testing.
Common parts of the workup include:
- Visual assessment to understand how severely vision is affected.
- Slit-lamp examination to look for corneal clouding, inflammation, and hypopyon.
- Sampling of aqueous or vitreous fluid for culture.
- Blood and urine cultures when endogenous infection is suspected.
When the back of the eye cannot be seen clearly because of dense inflammation, ultrasound can help detect vitreous debris, retinal detachment, or an intraocular foreign body in trauma cases. In real-world care, treatment is often started before culture results are available because waiting can worsen the visual outcome.
Treatment Options Explained
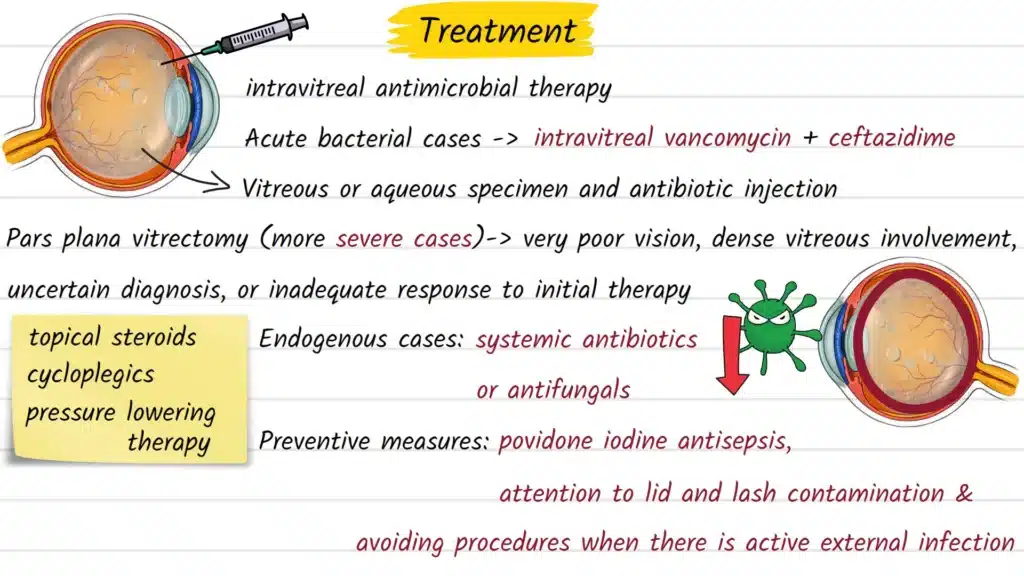
Treatment is urgent and usually starts with antimicrobial medication injected directly into the eye, because this reaches the site of infection more effectively than eye drops alone in many cases. Major references list broad-spectrum intravitreal antibiotics such as vancomycin and ceftazidime as common initial therapy while test results are pending.
Some patients also need surgery called a vitrectomy, which removes infected vitreous material from inside the eye. ASRS notes that this is especially important when vision is already very poor at presentation or when the amount of infectious debris is substantial.
Treatment may include:
- Intravitreal antibiotics or antifungal medication.
- Vitrectomy in selected or severe cases.
- Intravenous treatment when the infection is thought to have spread through the bloodstream.
- Supportive medications, such as corticosteroids in some situations, depending on the overall clinical picture.
The exact plan depends on the likely source, the suspected organism, the patient’s vision, and whether the infection is exogenous or endogenous. This article is informational only, and treatment choices must be made by a qualified ophthalmologist or retina specialist.
Possible Complications if Left Untreated
Untreated endophthalmitis can lead to irreversible vision loss. In rare cases, infection can spread beyond the eye to involve surrounding structures and even the central nervous system.
Even with prompt treatment, visual prognosis can still be guarded, especially in severe or traumatic cases. Outcomes often depend on how quickly treatment begins, the type of organism involved, and how much inflammation is already present when the patient is first examined.
Prevention and Risk Reduction
Not every case can be prevented, but risk reduction is part of modern ophthalmic care. Most exogenous cases are linked to surgery, injections, or trauma, which is why sterile technique, careful wound management, and prompt treatment of eye injuries matter.
Patients can reduce delays in care by seeking urgent review after eye surgery or eye injections if they notice new pain, redness, light sensitivity, or worsening vision. After eye trauma, especially when metal, plant material, or dirt may have entered the eye, same-day specialist assessment is important because retained foreign material raises the risk of infection.
When to See an Eye Doctor
Seek urgent ophthalmic care the same day for sudden vision loss, significant eye pain, marked redness, or rapid worsening after eye surgery, an eye injection, or eye injury. Endophthalmitis is considered an emergency, not a condition to watch at home for a few days.
People with fever, sepsis, recent hospitalization, or known bloodstream infection who also develop eye pain or vision changes should be assessed promptly because endogenous spread is possible. Fast evaluation does not guarantee a full recovery, but it gives the best chance of protecting vision.
Frequently Asked Questions
It often causes severe eye pain, redness, decreased vision, and sensitivity to light.
Yes. Major medical references describe it as a medical emergency because vision prognosis is closely linked to how quickly treatment starts.
Yes. One of the most recognized forms is postoperative endophthalmitis after eye surgery, including cataract procedures.
Yes. Endogenous endophthalmitis occurs when infection reaches the eye through the bloodstream from another part of the body.
Diagnosis is based on urgent eye examination and testing of fluid samples from the eye, often with additional blood or urine cultures when systemic infection is suspected.
No. Some patients are treated with urgent injections into the eye, while others need vitrectomy depending on vision, severity, and the clinical scenario.
Recovery varies. Some eyes do better than others, but even with early treatment the visual outcome can still be poor in severe cases.