Orbital cellulitis is a serious eye related infection that can threaten both vision and life if it is not treated quickly. It affects the tissues located deep inside the eye socket, behind the eyelids, and often develops as a complication of sinus infections or other nearby infections. Because orbital cellulitis can be difficult to distinguish from milder conditions such as preseptal cellulitis, understanding the key differences, warning signs, and treatment options is essential for patients, parents, and healthcare professionals.
This article explains what orbital cellulitis is, how it differs from preseptal cellulitis, the most common causes, symptoms you should never ignore, and how doctors diagnose and treat this condition.
What Is Orbital Cellulitis?
Orbital cellulitis is a serious bacterial infection that affects the tissues behind your eye, inside the bony cavity known as the orbit. The orbit is the bony socket where your eyeball sits. Inside this space are the muscles that move the eye, the fat that cushions it, blood vessels, nerves, and other soft tissues. Orbital cellulitis does not usually involve the eyeball itself, but it spreads within this confined space around the eye, which is why it can become dangerous very quickly.
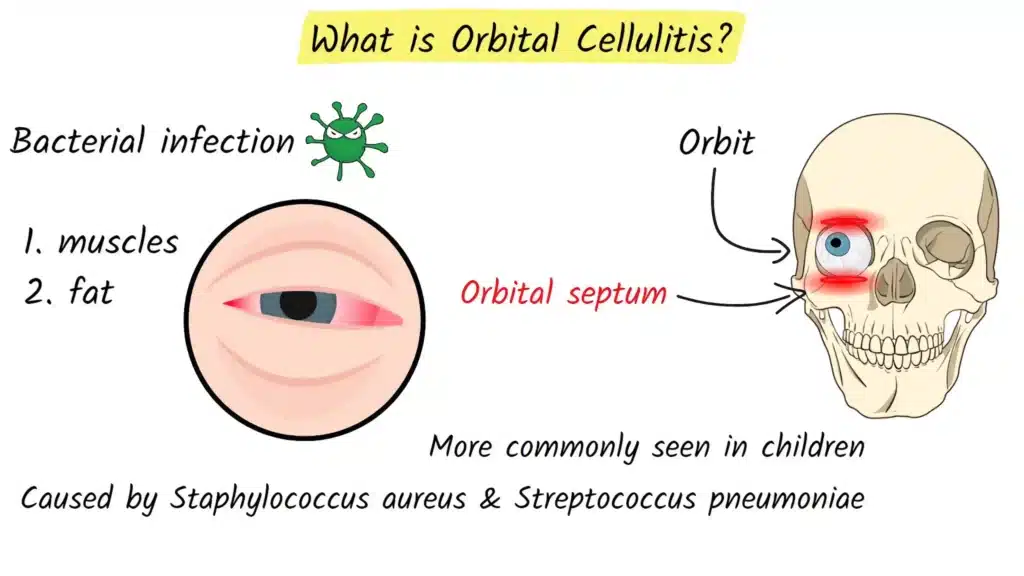
A key structure involved in understanding orbital cellulitis is the orbital septum. The orbital septum is a thin layer of tissue that acts like a protective wall between the front of the eyelids and the deeper tissues of the orbit. Infections that remain in front of this barrier are usually less serious. Once bacteria cross this barrier and enter the orbital space behind it, the infection is classified as orbital cellulitis and becomes an emergency.
Orbital cellulitis is more commonly seen in children, but it can affect adults as well. The most frequent bacteria responsible for this condition include Staphylococcus aureus and Streptococcus pneumoniae, along with other streptococcal species. These organisms often start in nearby areas, such as the sinuses, and then spread into the orbit.
Preseptal vs Orbital Cellulitis
Preseptal cellulitis and orbital cellulitis can appear similar at first glance because they both cause redness and swelling around the eye. However, they are very different in terms of severity and the tissues they involve. Knowing how they differ is important, because orbital cellulitis requires urgent hospital treatment, while preseptal cellulitis is usually managed more simply.
Preseptal cellulitis, also called periorbital cellulitis, affects only the eyelid and the surrounding skin in front of the orbital septum. In this condition, the infection is limited to the more superficial tissues. The eyelid looks red, puffy, and tender. Patients may feel uncomfortable, but their actual eye movements remain normal, their vision is not affected, and moving the eye does not cause pain. In many cases, preseptal cellulitis can be treated successfully with oral antibiotics and close follow up, especially if there are no signs that the infection is spreading deeper.
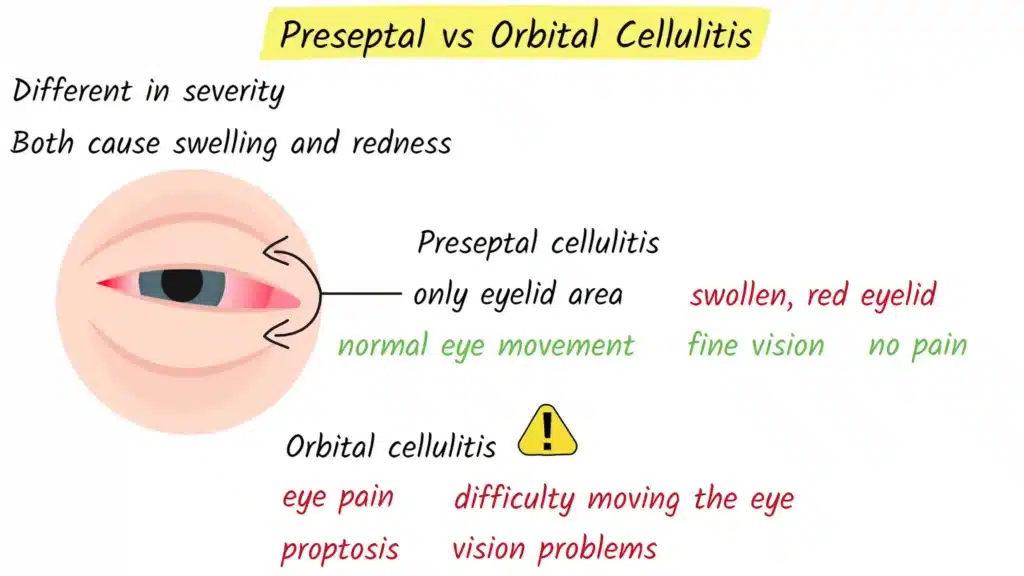
Orbital cellulitis, on the other hand, occurs behind the orbital septum and involves the deeper structures of the orbit. This is why it is considered a true medical emergency. When the infection reaches this space, it can affect the muscles that move the eye, compress the optic nerve, and potentially spread to the brain. The key signs that suggest orbital cellulitis rather than preseptal cellulitis include pain when moving the eye, difficulty moving the eye in different directions, bulging of the eyeball, and vision changes. These features indicate that the infection has gone beyond the eyelid and started to compromise the tissues within the orbit.
If a patient presents with a red, swollen eyelid, doctors look very carefully for these red flag signs. The presence of eye movement pain, reduced eye movements, proptosis, or changes in vision usually prompts immediate imaging and hospital admission for intravenous antibiotics.
What Causes Orbital Cellulitis?
The most common cause of orbital cellulitis is a bacterial sinus infection that spreads into the orbit. The sinuses are air filled spaces within the bones of the face and skull, located around the nose and eyes. The ethmoid sinuses, in particular, sit directly next to the orbit and are separated from it by a very thin piece of bone. In children, this bone can be especially thin, which makes it easier for bacteria from an infected sinus to cross into the orbital space.
When sinusitis becomes severe or is not adequately treated, bacteria can break through this bony barrier or travel through small blood vessels into the orbit. This is why many patients with orbital cellulitis have a history of recent or ongoing sinus infection, often with nasal congestion, facial pain, or headache before eye symptoms start.
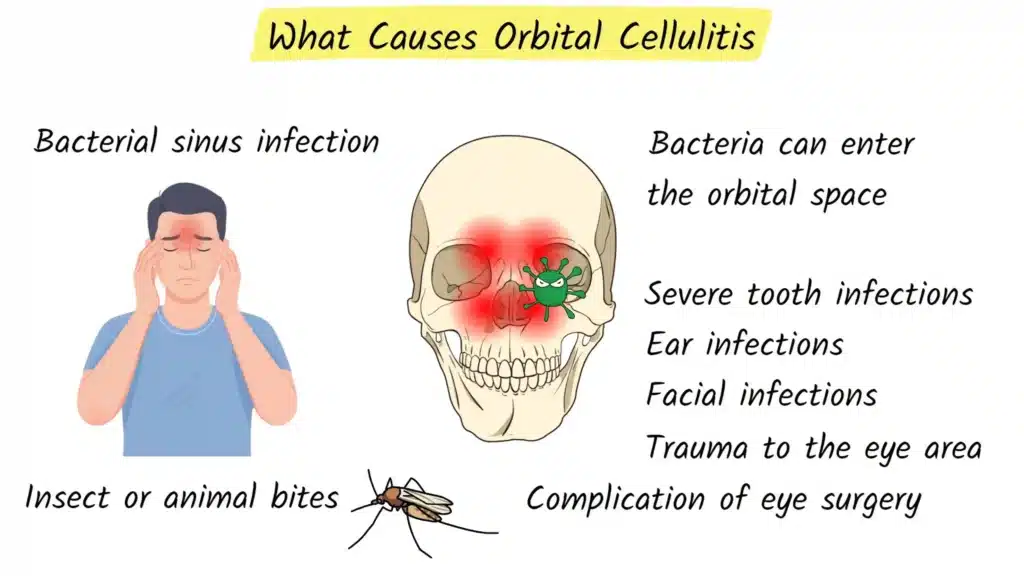
Orbital cellulitis can also develop from other sources. Severe tooth infections, especially in the upper jaw, can spread into the maxillary sinus and from there into the orbit. Ear infections or skin infections on the face and eyelids can extend deeper if they are not controlled in time. Trauma around the eye, such as a fracture of the orbital bones, a penetrating injury, or a foreign object, can introduce bacteria directly into the orbital tissues. Even insect or animal bites near the eye can be a starting point for infection if bacteria are carried into the tissue. In some cases, orbital cellulitis appears as a complication after eye or sinus surgery, particularly if there is postoperative infection.
People with weakened immune systems, such as those with poorly controlled diabetes or those taking immunosuppressive medications, may be at higher risk because their bodies have more difficulty containing infections before they spread.
Symptoms of Orbital Cellulitis
Doctors often talk about the three classic warning signs of orbital cellulitis, sometimes referred to as the three P’s. These are pain with eye movement, proptosis, and problems with eye movement.
Pain with eye movement is often one of the earliest clues that the infection has gone behind the orbital septum. Even gentle attempts to look up, down, left, or right can trigger sharp or deep aching pain. Proptosis is the medical term for forward displacement of the eyeball. When proptosis is present, the affected eye may look like it is bulging forward compared with the other eye, or the eyelids may not close comfortably over the eye because of swelling and pushing from behind. The third P is problems with eye movement. The eye may not move fully in all directions, may feel stiff, or may move only with significant pain. These features strongly suggest deeper involvement of the orbital structures rather than a simple eyelid infection.
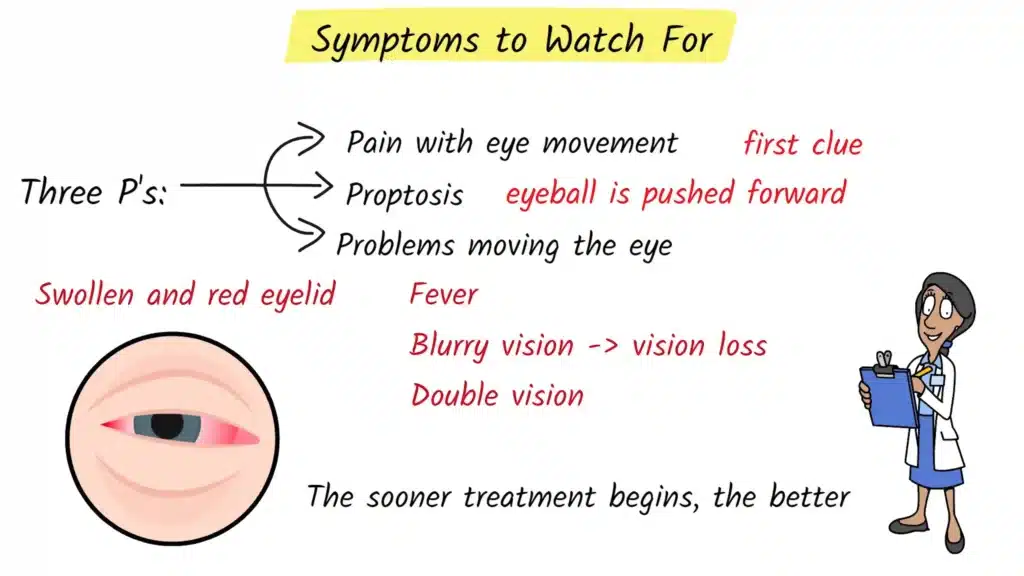
Beyond these three key signs, patients with orbital cellulitis typically have a very swollen and red eyelid, often to the point where the eye can be difficult to open. The area around the eye may feel warm, firm, and extremely tender to touch. Fever is common, and many patients feel generally unwell, with fatigue, chills, or headache. Vision can be affected, ranging from mild blurring to more serious loss of visual clarity. Some patients notice double vision because the eyes are not aligned properly when one eye cannot move as it should.
It is especially important to seek immediate medical attention if these symptoms occur after a recent sinus infection, tooth infection, facial infection, or trauma to the eye area. Orbital cellulitis can progress rapidly, so early evaluation and treatment greatly improve the chances of a full recovery.
How Orbital Cellulitis Is Diagnosed
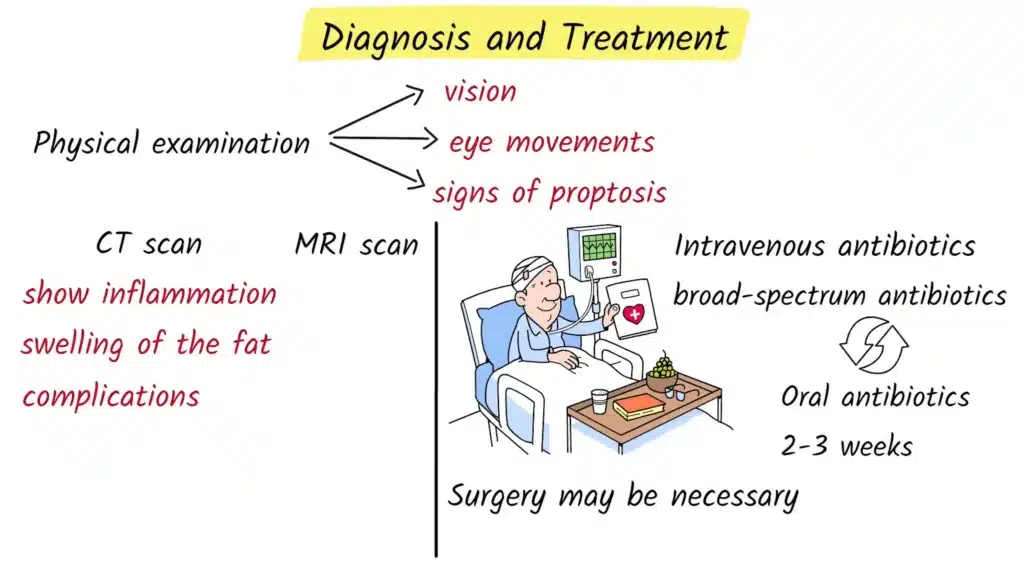
When a patient arrives at the hospital with suspected orbital cellulitis, the evaluation starts with a careful physical examination. The doctor will check visual acuity to see how clearly the patient can read letters or symbols on a chart. Eye movements are tested in all directions to see whether they are limited or painful. The doctor also looks for signs of proptosis, eyelid swelling, and redness, and examines the pupils and, if possible, the back of the eye to look for signs of pressure on the optic nerve.
Because preseptal and orbital cellulitis can look similar in the early stages, imaging is usually needed to confirm the diagnosis and determine how deep the infection has spread. The most commonly used imaging test is a CT scan of the orbits and sinuses. A CT scan can quickly show thickening of the eye muscles, swelling of the orbital fat, areas of fluid that might represent abscesses, and involvement of the surrounding sinuses. In some cases, especially if there is concern about spread to the brain or the cavernous sinus, an MRI scan may also be performed, as it can provide more detail of soft tissues and intracranial structures.
Blood tests are often taken to look for markers of infection, such as an elevated white blood cell count or increased inflammatory markers. Depending on the situation, doctors may also take cultures from the sinuses, a wound, or blood samples to identify the exact bacteria causing the infection, which allows them to tailor antibiotic therapy more accurately.
Treatment of Orbital Cellulitis
Orbital cellulitis is always treated as a medical emergency. Most patients need to be admitted to the hospital so that treatment can start quickly and the condition can be monitored closely. The main treatment is intravenous antibiotics. Giving antibiotics directly into a vein allows the medication to reach high levels in the blood and infected tissues much faster than with tablets.
Doctors usually start with broad spectrum intravenous antibiotics that cover the most likely bacteria, including common sinus pathogens, staphylococcal species, and sometimes anaerobic bacteria, especially if a dental source is suspected. Once culture results or other test findings are available, the antibiotic regimen may be adjusted to target the specific organisms involved. Patients typically receive intravenous antibiotics for several days, and doctors look for signs of improvement such as reduced fever, decreasing swelling, less pain, and better eye movement.
After there is clear clinical improvement, patients are usually switched from intravenous to oral antibiotics. These are continued at home for a total treatment course of around two to three weeks, depending on the severity of the infection and the patient’s overall health. Completing the full course is important to prevent relapse or incomplete resolution.
In some situations, surgery is required. If imaging shows a well defined abscess in or around the orbit, or if vision is threatened by pressure on the optic nerve, surgical drainage may be necessary. Surgeons may also operate on the sinuses to drain infected material and restore normal sinus drainage. These procedures are often performed by an ear, nose, and throat specialist, sometimes in collaboration with an ophthalmologist. Surgery is also considered if there is no improvement after twenty four to forty eight hours of appropriate intravenous antibiotics, or if there are signs that the infection has spread toward the brain or cavernous sinus.
Complications and Recovery
Without prompt treatment, orbital cellulitis can cause serious complications. One of the most feared is permanent vision loss. This can occur if the infection compresses the optic nerve, cuts off blood supply to the eye, or causes severe inflammation around the nerve. The confined space of the orbit means that even a small increase in pressure can have big consequences for the delicate structures inside.
The most dangerous complication occurs when the infection spreads to the cavernous sinus, which is a large vein located at the base of the brain. This condition, called cavernous sinus thrombosis, is life threatening and requires immediate intensive treatment. The infection can also spread to the coverings of the brain, causing meningitis, or into the brain tissue itself, leading to a brain abscess. These complications may present with severe headache, neck stiffness, confusion, seizures, or other neurological symptoms.
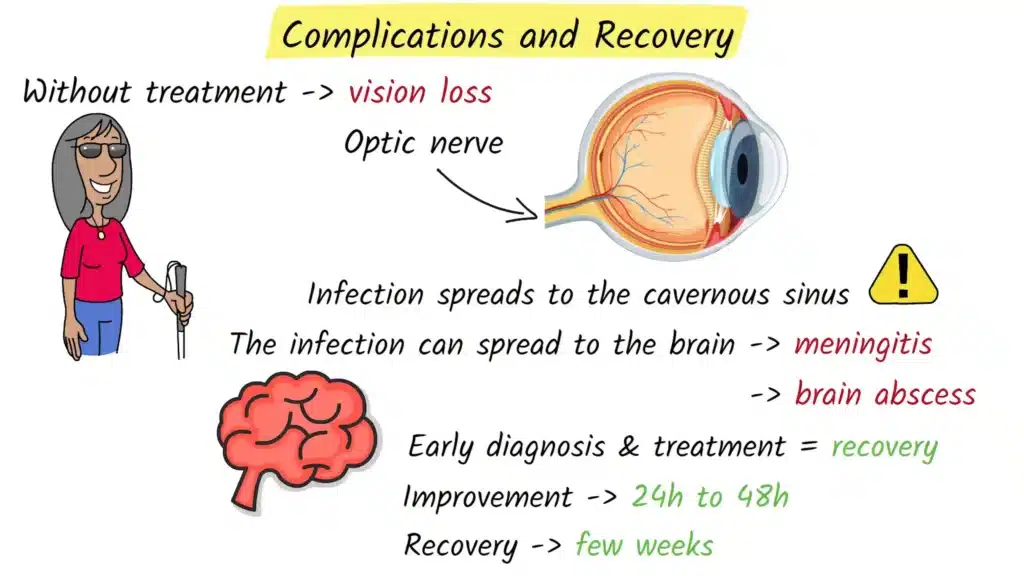
The good news is that with early diagnosis and appropriate antibiotic therapy, most people recover completely from orbital cellulitis. Many patients begin to show improvement within twenty four to forty eight hours after starting intravenous antibiotics. Swelling and redness gradually decrease, pain lessens, and eye movements and vision often return to normal over the following days and weeks. Full recovery can take several weeks, especially in more severe cases or when surgery has been required. Follow up with an ophthalmologist is important to make sure that vision has fully recovered and that there are no long term complications.
References
Danishyar, A., & Ashurst, J. V. (2023). Orbital Cellulitis. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK507901/
BlueFin Vision. (2026). What Is Orbital Cellulitis? https://bluefinvision.com/blog/what-is-orbital-cellulitis/
All About Vision. (2021). Orbital Cellulitis: Symptoms, Causes and Treatment. https://www.allaboutvision.com/conditions/infections-allergies/cellulitis/orbital/
Eyes On Eyecare. (2025). Periorbital vs Orbital Cellulitis. https://eyesoneyecare.com/resources/periorbital-vs-orbital-cellulitis-concise-walkthrough-cheat-sheet/